Download
1 / 40
400 likes | 539 Views
Why NMEs and Therapeutic Biological Products Fail in the First FDA Review Cycle. Partha Roy, Ph.D. | April 24, 2013. Positive Impact of PDUFA (1). Positive Impact of PDUFA (2). NMEs 1st cycle approval rates in the past 3 years . . . by APPROVAL Cohorts.

E N D
Why NMEs and Therapeutic Biological Products Fail in the First FDA Review Cycle Partha Roy, Ph.D. | April 24, 2013
NMEs 1st cycle approval rates in the past 3 years . . . by APPROVAL Cohorts Distribution of Review Cycles to Approval / NMEs (and BLAs) Approved in 2010 – 2012 • 76% of approved NMEs cleared in 1st review cycle 2010 – 2012 • 61% of approved BLAs cleared in 1st cycle 2010 – 2012
NME (CDER) vs. Therapeutic Biologic (CDER) vs. Non-Therapeutic Biological* (CBER) Product Approval Times, 2005 – 2012+ 2 *Vaccines, blood products, gene/cell therapies 1excluding 78.0-month review of Asclera 2excluding 94.8-month review of Surfaxin +through July 2, 2012
CDER-wide Performance on Original NDAs Percent of NDAs Receiving Approval, Complete Response, and Withdrawal Actions FY1997 – FY2011** Many-year high Record pace *as of December 31, 2009, when 118 of 120 FY2008 NDAs had received first actions **as of April 30, 2012, when 64 of 91 FY2011 NDAs had received first actions
Priority NDA review outcomes overall:Heavily tilted to “positive” outcomes…… Percent of Priority NDAs Receiving Approval, Complete Response, and Withdrawal Actions, FY1998 – FY2011 Will be new record * as of April 30, 2012, when 17 of 18 FY2011 priority NDAs had received first actions
Standard NDAs sidetracked more often until recently… Percent of Standard NDAs Receiving Approval, Complete Response, and Withdrawal Actions, FY1997-FY2011 At least many-year high Standard NDAs: Recent uptick in 1st cycle approval rate *as of December 31, 2009, when 91 of 93 FY2008 standard NDAs had received first actions; **as of April 30, 2012, when 47 of 73 standard NDAs had received first actions.
First-in-Class (FIC) NMEs/NBEs Distribution of Review Cycles to Approval FIC NMEs/NBEs Approved in 2011 and 2012 • 78% of FIC NME/NBEs cleared in 1st cycle vs. 73% of all NME/NBEs (among 2011/2012 approvals) • 85% of 2012 FIC NME/NBEs cleared in 1st cycle • 62% of FIC NME/NBE approvals were priority-rated (only 50% of 2012) vs. 47% of all NME/NBEs (2011/2012 approvals) • Of 32 FIC medicines, 11 are oncology
Is There a Review Time Advantage for First-in-Class(FIC) NMEs/NBEs? FIC NMEs/NBEs Approved 2011 – 2012 (1H) * drops to 9.5 months if Firazyr's45.9-month review is excluded. Rises to 14.2 months if three cancer NMEs (Zytiga, Zelboraf, Xalkori) are excluded. ** only 7 of the 25 non-FIC products were priority-rated vs. 14 of 17 of the first-in-class products. + excluding 94.8-month review of Surfaxin. Rises to 18.4 months if Surfaxin is included.
Reasons Why BLAs Fail in 1st Review Cycle 2 Issues Potiga3 1 Issue 3+ Issues Daliresp2 Nulojix 1) Efficacy was repeatedly identified as primary issue; 2) CRL listed 3 issues preventing approval, 1 of which not identified (redacted). Two others were safety related. Implication was other was safety-related as well, but not clear. There appeared to be consensus that safety was a key issue, but disagreement about whether efficacy was an issue. 3) Primary CR reason was high-specification limit for mutagenic impurity (called "chemistry/carcinogenicity issue"). Also, "less important deficiency" was potential to cause urinary symptoms. 4) Clinical Reviewer noted that “major deficiencies” were clinical in nature (need for a reader training process suitable for marketplace).
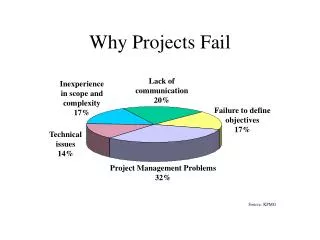
Where is the NDA Workload Heading? Top Divisions by FY 2011 NDA Submissions Others: Anti-Infective (5), Cardiovascular and Renal (5); Anesthesia, Analgesia and Addiction (4); Dermatology/Dental (4); Medical Imaging (2); Psychiatry (2); Transplant/Ophthalmic (2); Nonprescription Clinical Evaluation (1)
Gap Analysis: Just How Much is a Priority Rating Worth? Priority/Standard NME Review Gap, 1995-2012* (in months) 1 Excludes outlier Multaq (48.7 months) and Sabril (19.8 months). If these were included, 2009 priority mean would jump to 18.5 months. 2 Drops to 6.8 months if 34.7 month review of Xenazine is excluded. 3 Excludes outlier Asclera review (78.0 months). 4 In calculating 2009 standard NME mean, we excluded one outlier (Sabril, at 182.6 months). 5 Drops to 8.7 months if 45.9-month review of Firazyr is excluded. 6Drops to 4.1 months if 19.6-month Amyvid review is excluded. 7Excluding 94.8-month review of Surfaxin * through July 25, 2012
The review gap holds up in most divisions... The Priority vs. Standard Review Time Gap | Selected Divisions * Excludes 78.0- month review of Asclera and 48.7- month review of Multaq + includes 18.5- month review of Effient
Priority / Standard Therapeutic Biologic Review Gap Mean Review Time for Therapeutic Biologics: 2007 – 2012** (In Months) *Includes 23.8-month review of Lumizyme and 22.5-month review of Krystexxa **Through August 6, 2012
In reality, how many NDAs get to join this elite class? Percent of All Submitted NDAs Obtaining Priority Review Status FY1997-FY2011
Divisional priority designation rates: Who are the givers? Percent of Original NDA Submissions FY2005-FY2008 Granted Priority Status | A Division-by-Division Analysis Gaining priority status a fight outside of HIV/Cancer
Divisional priority designation rates: Who are the givers? Percent of Original NDA Submissions FY2009 – FY2011 Granted Priority Status | A Division-by-Division Analysis Priority Rates in Oncology and Antiviral Recover in FY2011 * FY2011 data only; **FY2009/FY2010 data only
Why Are NMEs Failing in the 1st Review Cycle? • Booz Findings, 2008: Tilted Slightly Toward Efficacy as Most Frequent Deficiency • PAREXEL, 2012: Tilted Heavily Toward Safety • CMC and Efficacy Next-Most Common Reasons (PAREXEL) • Dose-Related Issues Apparent for About 40% of 1st Cycle Failures • Almost Two-thirds of Resubmitted NDAs Succeeding Today (Class 2)
Reasons Why NMEs Fail in 1st Review Cycle 1 Issue 2 Issues Belviq Saphris Arcapta Neohaler4 Uloric Potiga9 Sabril8 Natroba Daliresp3 3+ Issues Brilinta Xarelto Horizant Vibativ Ulefsia Elelyso Asclera5 SAMSCA DaTscan Fanapt7 Ferriprox2 Multaq6 1) Efficacy was repeatedly identified as primary issue. 2) CRL had 29 deficiencies/requests (11 under clinical, 3 under clinical pharmacology, and 15 under product quality). 3) CRL listed 3 issues preventing approval, 1 of which not identified (redacted). Two others were safety related. Implication was other was safety-related as well, but not clear. There appeared to be consensus that safety was a key issue, but disagreement about whether efficacy was an issue. 4) All dose-related issues. 5) Multiple issues, but efficacy called "the critical issue." ClinPharm/biopharmaceutics issue mentioned as well, but was more of a data integrity issue. 6) Multiple issues, but safety issue called "overwhelming impediment to drug approval." 7) Two "major deficiencies" identified, although four other issues needed addressing (considered "not reasons for not approvable action"). 8) Safety concerns called "most critical" to non-approval. While safety/efficacy concerns were main issues, approvable letter also requested biopharmaceutics information. 9) Primary CR reason was high-specification limit for mutagenic impurity (called "chemistry/carcinogenicity issue"). Also, "less important deficiency" was potential to cause urinary symptoms. 10) Clinical reviewer noted that “major deficiencies” were clinical in nature (need for a reader training program suitable for marketplace). 11) Cross discipline team leader review notes that “clinical recommendation for the original submission was Approval; however, there were major CMC deficiencies that led to “initial and subsequent review cycles.”
Reasons Why NMEs Fail in 1st Review Cycle (% of 25 Complete Response Letters Citing Area) 1 1missing financial disclosure forms
Safety Issues • Liver toxicity (clinical data insufficient to characterize) [Xarelto] • Inadequate assessment of CV/thrombotic safety signal/drug interactions [Uloric] • CV (QTcF interval lengthening)/imbalance of reported rate of renal and vascular disorders/teratogenicity/insufficient dosing info [Vibativ] • Cancer safety signal (in rat) [Horizant] • Cancer signals (unresolved exposure/response relationship in drug-emergent adenocarcinoma and “diagnostic uncertainty” in classification of mammary masses in rats) [Belviq] • Inadequate info on systemic bioavailability in children under 4yoa [Natroba (ped indication)] • Suicidality/psychiatric AEs/drug interactions (lack of substantial evidence of safety) [Daliresp] • Unsupported High Dose/CV-Cerebrovascular AEs/Asthma-related deaths [Arcapta Neohaler] • Little/no assessment of DVT (known class-specific concern) [Asclera] • Nonclinical testing insufficient to support chronic intermittent dosing/self-injection safety/ safety of same dose for different genders and ages/further definition of dose [Firazyr]
Safety Issues (continued) • Need to review nonclinical histopathology data from carcinogenicity study/concerns regarding anemia/thrombocytopenia AEs [Saphris] • High proposed spec . limit for mutagenic impurity*/potential to cause urinary symptoms [Potiga] • Insufficient safety data (lack of patient numbers at relevant doses) [Fanapt] • Insufficient safety data (to verify absence of mortality disadvantage w/ LT use, and to assess arrhythmogenic potential, signal of possible liver tox, supportive study had design/analysis features consistent with exploratory study) [Ferriprox] • Inadequate evaluation of immunogenic potential/LT data insufficient to assess chronic immune-mediated AEs associated w/ drug class [Elelyso] • Increase in mortality in CT of high-risk population and other “safety concerns,” including carcinogenicity, teratogenicity, and endocrine effects [Multaq] • Need to clarify significance of high/sporadic drug plasma concentrations in systemic exposure study [Ulefsia] • Inadequate reporting of AE data collection [Sabril] • *was primary issue, categorized as chemistry/carcinogenicity issue
Efficacy Issues • Regional differences (US vs. OUS) in CT efficacy results/use of post-facto explanation [Brilinta] • Insufficient justification of higher dose/appropriate dosing frequency [Arcapta Neohaler] • Drug superiority to active control not demonstrated in primary efficacy parameter/Non-inferiority to active control not established [Asclera] • Uncertain efficacy of comparator/concerns over validity of primary efficacy endpoint/lack of substantial evidence of efficacy of proposed dose [Firazyr] • Inadequate efficacy data—only one of four studies could be used to support efficacy (others included schizoaffective disorder, “a distinct entity”) [Fanapt] • Need for clinically applicable reader training materials/verification of reproducibility of image interpretations [Amyvid] • Concerns over marginal efficacy (in overweight and obese persons w/o type 2 diabetes) given safety findings (breast and brain tumors in rats) [Belviq] • Clinical data did not establish “clinical benefit attributed to primary endpoint”/primary endpoint result not “robust observation” due to small trial size/secondary endpoints not consistently corroborative of primary endpoint result/supportive study designed like an exploratory study [Ferriprox] • Drug’s immunogenic potential and impact on efficacy not adequately assessed/insufficient data to assess efficacy of drug in patients switched from other ERTs [Elelyso] • Decreased efficacy noted in patients with increased age and with decreased baseline creatinin levels [Vibativ] • Efficacy in one indication (partial seizures) not definitively demonstrated [Sabril]
Chemistry, Manufacturing and Controls (NMEs) Xarelto: 8 citations, including: • 3 involving inadequate DMFs • Insufficient drug substance information to confirm nomenclature, description, physicochemical properties, specifications, primary stability protocol, post-approval stability commitment, and primary stability data • Drug product specification inadequate (fails to propose analytical methods for test parameters) • Proposed acceptance criteria differ btw clinical trial sponsor and NDA applicant • Proposed acceptance criterion for dissolution not acceptable • Container/closure system not adequately described • Proposed stability study inadequate (no stability data submitted for pilot or commercial batches) Natroba: • Analytical method for assaying drug product not fully validated • “Drug product exhibits [redacted] during storage” • “Drug product has [redacted] problem during the accelerated conditions” Asclera: • “Controls inadequate to prevent micro-organisms surviving the sterilization procedures” Note: an additional CMC issue (it seems a change in manufacturer w/o inclusion of validation and requalification reports) resulted in RTF of NDA resubmission. Applicant took almost another year to resubmit the NDA addressing this issue.
Chemistry, Manufacturing and Controls (NMEs) (cont’d) Firazyr: 20 individual CMC deficiencies, including: • Inadequately qualified impurities • Stability data do not support requested expiration period (18 months) • Tightened acceptance criteria for residual solvent content, individual/total impurities, degradation products, and amino acid analysis needed • Post-approval stability protocols/stability commitment needed for drug substance • Upgraded proposed impurity specification needed • DMF issues (unspecified) • Revised stability protocol needed Vibativ: • “Significant [CGMP] deviations” found at manufacturing facility, all unspecified Ferriprox: 15 citations, mostly highly specific information requests under heading, “Product Quality.” The CRL citations/requests included the following: • Analytical method transfer docs not adequate (e.g., incomplete, studies summarized not sufficient for purpose) • System suitability criterion for drug substance and drug product differ without explanation • Deficient DMF (undisclosed deficiencies) • Warning letter issued for cGMP deficiencies at manufacturing facility (undisclosed deficiencies).
Chemistry, Manufacturing and Controls (NMEs) (cont’d) Ulefsia • Container/closure proposal “should be implemented” • Manufacturing facility deficiencies identified during FDA inspection must be addressed Potiga • High specification limit proposed for mutagenic impurity, which FDA said would result in a daily dose of the impurity considered unacceptable for a genotoxic impurity. Zioptan • Lone issue was failure to prove assurance of product’s sterility. CRL noted that, although applicant revised its “[redacted] processing validation protocol” in an NDA amendment, the agency would need a report describing “three consecutive successful [redacted] processing simulations [redacted]” employing the new protocol before approval. Amyvid • Unspecified manufacturing facility deficiencies identified during FDA inspection • Product quality issues, largely labeling (bulk product vial label, carton label, package insert) Surfaxin (multiple review issues): 31 different FDA “comments,” although the critical issues were summarized in the CDTL review as follows: • Drug substance-related impurities exceeding ICH-recommended qualification threshold • “Major deficiencies” related to inadequate specifications for release and stability, inadequate info on manufacturing process, inadequate stability data, inadequate acceptance criteria for impurities, and inadequate validation of the lucinactant bioassay to be used for lot release testing.
Chemistry, Manufacturing and Controls (NMEs) (cont’d) Elelyso: CRL had 34 CMC-related issues in three categories: • Product Quality (specifications and assay validation, comparability, process validation, and control of impurities); 17 deficiencies, including: • results of particulate testing and appearance testing of reconstituted drug needed • need to identify/control for quantity of variants to establish control strategy • monosaccharide content/glycan structure analysis contained inconsistent results • time limits for individual manufacturing steps and complete process not defined in NDA • Immunogenicity: 6 deficiencies, including: • employed assay insufficient to address drug tolerance at low concentrations of anti-product antibodies • Microbiology: 3 deficiencies/requests, including: • validation summary reports necessary for sterility and bacterial endotoxin test methods
Drilling Down on the Data: Mind the Dose • Dose-related issues were important in ~40% of complete response letters. • Issues ranged from failure to explore full dose range, to lack of safety exposure data in proposed dose range, to failure to show higher doses provide “any greater benefit” than lower doses. • In some cases, dose is the issue even when it does not appear to be. Horizant: • Primary concern: carcinogenicity (finding in rat) • FDA: wanted additional trial to determine lowest effective dose • Reason: Identify if lower dose would provide greater margin of safety and “might justify approval”
Why are BLAs (Therapeutic Biologics) Failing in the1st Review Cycle? • NMEs = Heavily Tilted Toward Safety Issues (PAREXEL, 2012) • BLAs = CMC/Product Quality Issues Dominate (PAREXEL, 2012) • CMC/Product Quality was a Key Issue in 78% (7 of 9) of the Cases • Safety was a Key Issue in 67% of the Cases • REMS was Identified as a Key Issue in 75% of the Cases
Reasons Why BLAs Fail in 1st Review Cycle Stelara2 1 Issue 3+ Issues Nulojix Kalbitor Raxibacumab6 Actemra Krystexxa1 Lumizyme 1 Two separate CMC issues. 2 Safety = REMS. 3 There was a third deficiency that was not identified. 4 One deficiency not disclosed (redacted in full). 5Complete response letter listed "reasons for this action" in two categories: (1) "Deficiencies" (data integrity, CMC (device, pre-filled syringe), safety (reproductive toxicity), nomenclature, and undisclosed deficiency); and (2) "Information Requests" (characterization of potential for binding and neutralizing anti-product antibodies, characterization of critical attributes and narrowing of specifications, information on pediatric use, and potential to prolong the QT interval). 6 Efficacy based on animal studies (inhalation anthrax). CRL had a number of “additional requests” (not “deficiencies”) in clinical and product quality areas.
Product Quality/Manufacturing Issues (NBEs) Krystexxa: 19 PQ/CMC deficiencies, the major deficiencies including: • Product made through commercial process not representative of Phase 3 material • Inadequate substance/product release testing program (e.g. , tighter accept. criteria) • Inadequate stability program for reference standard • Unsatisfactory pre-license inspection (drug substance manufacturer facility) Nulojix: Issues cited under two separate categories: • Product quality deficiencies (regarding “drug substance manufacturing,” but all additional information redacted) • Product quality microbiology deficiencies (inadequate container closure integrity test, shipping validation, drug product endotoxin specification, and labeling, other information redacted) Note: deficiencies “conveyed” following pre-license inspection of two facilities required resolution before approval, FDA noted Actemra: Unspecified deficiencies that were “conveyed” following pre-license inspection of manufacturing facility, and that FDA noted needed “satisfactory resolution” before approval
Product Quality/Manufacturing Issues (NBEs) Lumizyme: Two categories of PQ/CMC issues were noted: • Undisclosed “persistent..manufacturing facility deficiencies” leading to Warning Letter • “Product quality (CMC) deficiencies” related largely to several “critical product attributes that differed” between Lumizyme (produced at a 2000 L bioreactor scale) and Myozyme, also an alglucosidasealfa product made by Genzyme but a product that was already marketed and that was being produced at a 160L scale. FDA reviewers were concerned that the differences could contribute to differences in potency, immunogenicity, and decreased efficacy. Kalbitor: 9 of 11 deficiencies and “recommendations” in CRL address product quality, including: • Insufficient information on depyrogenation of 2 mL vials • Additional study for stopper sterilization needed • Deficient proposed protocol for assessing qualification of new working cell bank • Info on an assay’s Limit of Detection has not been submitted • Sensitivity of dye ingress container-closure integrity test not provided Note: CRL also cited deficiencies regarding release/stability specs, SDS-PAGE analysis, RP-HPLC assay specs, assay acceptance criteria, need for an identity test at a contract manufacturer responsible for fill/finish, and insufficient stringency of acceptance criteria in a reference standard qualification protocol to control potential drift in the reference standard’s characteristics.
Product Quality/Manufacturing Issues (NBEs) Stelara: CRL cited two key “product quality deficiencies” preventing approval: • Need for establishment of control procedures to validate performance of manufacturing processes responsible for causing variability in drug product. • Lack of an accurate and Quality Control Unit-approved testing and sampling method for measurement of visible particular matter. Neutroval: CRL noted one product quality issue under “deficiencies” (another entire citation was completely redacted) and several issues under “information requests”: • Deficiency: Inadequate information concerning device closure system. • Information request: several, including need for additional data to support proposed changes in DS product to improve microbial control, and need for a plan for development of a validated assay for confirmation of anti-product antibodies identified by screening assay. Raxibacumab: CRL noted one product quality issue: • Bacterial endotoxin specification for final product is inadequate.
Selected Characteristics in Approved NMEs with1stCycle Failures (among 23 NMEs) • Sponsors averaged >3 meetings (pre-IND to pre-NDA) during development • At least 15 of 23 drugs had EOP2 meetings (one drug had 3 EOP2 meetings) • At least 19 of 23 drugs had pre-NDA meetings (one drug had 4 pre-NDA meetings) • At least 3 fast track drugs, 4 orphan drugs, 1 accelerated approval • At least 9 NMEs thought to have Special Protocol Assessments (SPA) granted during development (i.e., before 1st cycle review) • Sponsors for at least another 2 NMEs sought SPAs, but were denied
Multi-Cycle NMEs Known/Thought to be Granted SPAs 1 FDA documentation suggests, but does not definitively establish, that SPA was granted. FDA notes that, after a “special protocol review,” the protocols were revised as requested by the division. “The Division agreed that the revised study design and planned analysis of studies adequately address the objectives necessary to support a regulatory submission.” 2 While no clear FDA acknowledgment that request was granted, FDA stated that, “Proposed protocol, endpoints, and sample size acceptable with caveat that treatment difference should be clinically meaningful (Written communication, July 29, 2004).” 3 While documentation doesn’t clearly confirm SPA request granted, it does note that, “The division agreed with the two-arm (1200 mg vs. placebo) trial.”
Multi-Cycle NMEs Known/Thought to be Granted SPAs(continued) 4 FDA said, “the design of the two pivotal studies was the subject of an SPA procedure.” 5SPA implied given multiple meetings of Executive Carcinogenicity Assessment Committee (CAC), and full CAC agreed that carcinogenic potential adequately tested, although additional testing recommended (not all CAC reviews have SPAs). 6 appears SPA granted on 10/26/2004. 7FDA documentation does not confirm SPA granted, but implied by saying, “clarification of recommendations made in SPA.” But SPA was with DMEP, before IND transferred to DCRP.
Disagreements/Failure to Follow FDA Advice (from FDA perspective)
Questions? Thank you