Download
1 / 1
10 likes | 141 Views
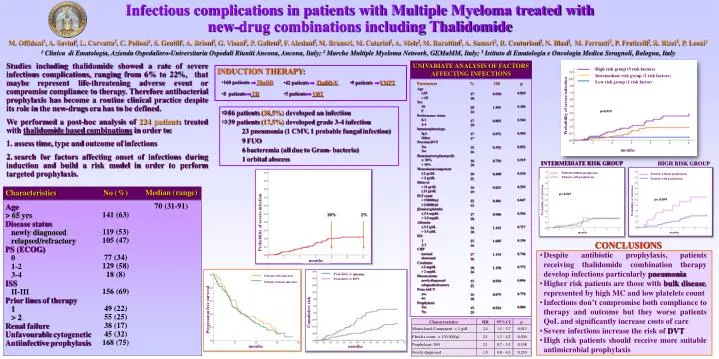
High risk group (3 risk factors). Parameters Age 65 > 65 Sex M F Performance status 0-1 2-4 Immunophenotype IgA Other Previous DVT Yes No Bone marrow plasmacells 30% > 30% Monoclonal component 2 gr/ dL > 2 gr/ dL Hb level < 11 gr/ dL 11 gr/ dL

E N D
High risk group (3 risk factors) Parameters Age 65 > 65 Sex M F Performance status 0-1 2-4 Immunophenotype IgA Other Previous DVT Yes No Bonemarrowplasmacells 30% > 30% Monoclonalcomponent 2 gr/dL > 2 gr/dL Hblevel < 11 gr/dL 11 gr/dL PLT count < 130000/ml 130000/ml b2-microglobulin 3.5 mg/dL > 3.5 mg/dL Albumin 3.5 g/dL > 3.5 g/dL ISS 1 2-3 CRP normal abnormal Creatinine 2 mg/dL > 2 mg/dL Disease status newlydiagnosed relapsed/refractory Prior ASCT yes no Prophylaxis Yes No % 17 18 20 14 17 20 17 17 32 16 16 20 10 21 16 19 22 12 17 18 16 18 23 16 17 16 18 16 13 22 16 18 15 25 OR 0.920 1.583 0.803 0.972 0.392 0.756 0.408 0.823 0.481 0.980 1.143 1.605 1.134 1.150 0.554 0.875 0.524 p 0.820 0.200 0.560 0.950 0.052 0.519 0.520 0.593 0.047 0.956 0.717 0.196 0.746 0.772 0.096 0.770 0.084 Intermediate risk group (2 risk factors) Low risk group (1 risk factor) Probability of severe infection Median (range) 70 (31-91) Characteristics Age > 65 yrs Disease status newlydiagnosed relapsed/refractory PS (ECOG) 0 1-2 3-4 ISS II-III Priorlinesoftherapy 1 > 2 Renalfailure Unfavourablecytogenetic Antiinfectiveprophylaxis No (%) 141 (63) 119 (53) 105 (47) 77 (34) 129 (58) 18 (8) 156 (69) 49 (22) 55 (25) 38 (17) 45 (32) 168 (75) Probability of severe infection months Infectious complications in patients with Multiple Myeloma treated with new-drug combinations including Thalidomide M. Offidani1, A. Savini1, L. Corvatta2, C. Polloni1, S. Gentili1, A. Brioni3, G. Visani2, P. Galieni2, F. Alesiani2, M. Brunori, M. Catarini2, A. Mele2, M. Burattini2, A. Samori2, R. Centurioni2, N. Blasi2, M. Ferranti2, P. Fraticelli2, R. Rizzi2, P. Leoni1 1 Clinica di Ematologia, Azienda Ospedaliero-Universitaria Ospedali Riuniti Ancona, Ancona, Italy; 2 Marche Multiple Myeloma Network, GEMaMM, Italy; 3 Istituto di Ematologia e Oncologia Medica Seragnoli, Bologna, Italy HIGH RISK GROUP • Studies including thalidomide showed a rate of severe infectious complications, ranging from 6% to 22%, that maybe represent life-threatening adverse event or compromise compliance to therapy. Therefore antibacterial prophylaxis has become a routine clinical practice despite its role in the new-drugs era has to be defined. • We performed a post-hoc analysis of 224 patients treated with thalidomide based combinations in order to: • assess time, type and outcome of infections • search for factors affecting onset of infections during induction and build a risk model in order to perform targeted prophylaxis. UNIVARIATE ANALYSIS OF FACTORS AFFECTING INFECTIONS p=0,023 18% 2% p= 0,004 Probabilityofinfection 86 patients (38,5%) developed an infection • 39 patients (17,5%) developed grade 3-4 infection 23 pneumonia (1 CMV, 1 probable fungal infection) 9 FUO 6 bacteremia (all due to Gram- bacteria) 1 orbital abscess months INTERMEDIATE RISK GROUP Patientswithoutprophylaxis Patientswithprophylaxis Patientswithoutprophylaxis Patientswithprophylaxis p= 0,921 Probabilityofinfection Patientswithinfection months Patientswithoutinfection months CONCLUSIONS • Despite antibiotic prophylaxis, patients receiving thalidomide combination therapy develop infections particularly pneumonia • Higher risk patients are those with bulk disease, represented by high MC and low platelets count • Infections don’t compromise both compliance to therapy and outcome but they worse patients QoL and significantly increase costs of care • Severe infections increase the risk of DVT • High risk patients should receive more suitable antimicrobial prophylaxis Cumulative risk Progression free survival Probabilityofinfection ProbabilityofDVT months months INDUCTION THERAPY: • 160 patients ThaDD • 5 patients VDT • 9 patients VMPT • 42 patients ThaDD-V • 8 patients TD months