Download
1 / 1
10 likes | 213 Views
Breast Feeding and Infant Body-Facial Orientations Amongst Routinely Bedsharing and Solitary Sleeping Mother-Infant Pairs: Mother As A Hidden Regulator of Infant Behavior Ted Brown, Kristin Klingaman, Dan Stevenson, James J. McKenna Department of Anthropology, University of Notre Dame.

E N D
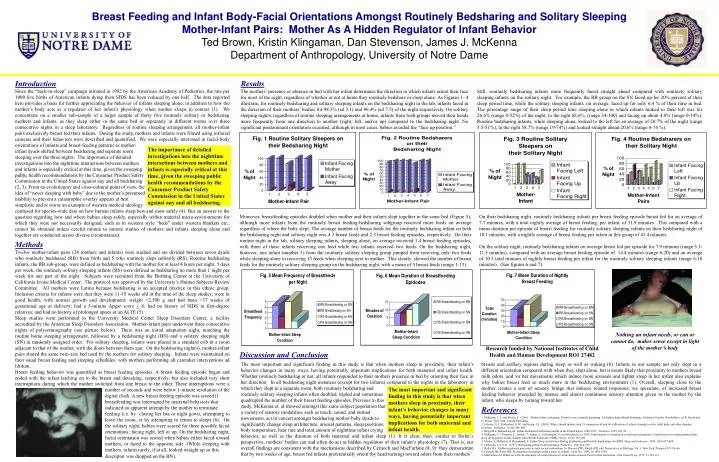
Breast Feeding and Infant Body-Facial Orientations Amongst Routinely Bedsharing and Solitary Sleeping Mother-Infant Pairs: Mother As A Hidden Regulator of Infant Behavior Ted Brown, Kristin Klingaman, Dan Stevenson, James J. McKenna Department of Anthropology, University of Notre Dame Introduction Since the “back-to-sleep” campaign initiated in 1992 by the American Academy of Pediatrics, the rate per 1000 live births of American infants dying from SIDS has been reduced by one half. The data reported here provides a basis for further appreciating the behavior of infants sleeping alone, in addition to how the mother’s body acts as a regulator of her infant’s physiology when mother sleeps in contact (1). We concentrate on a smaller sub-sample of a larger sample of thirty five routinely solitary or bedsharing mothers and infants, as they sleep either in the same bed or separately in different rooms over three consecutive nights in a sleep laboratory. Regardless of routine sleeping arrangement, all mother-infant pairs exclusively breast fed their infants. During the study, mothers and infants were filmed using infrared cameras and their behaviors were described and quantified. We were especially interested in facial-body orientations of infants and breast-feeding patterns as mother- infant dyads shifted between bedsharing and separate room sleeping over the three nights. The importance of detailed investigations into the nighttime interactions between mothers and infants is especially critical at this time, given the sweeping public health recommendations by the Consumer Product Safety Commission in the United States against any and all bedsharing (2, 3). From an evolutionary and cross-cultural point of view, the idea of “never sleeping with baby” due to the mother’s presumed inability to prevent a catastrophic overlay appears at best simplistic and at worse an example of western medical ideology confused for species-wide data on how human infants sleep best and most safely (4). But an answer to the question regarding how and where babies sleep safely, especially within material micro-environments for which they were not necessarily designed, such as in western style “beds” under western blankets etc., cannot be obtained unless careful minute to minute studies of mothers and infants sleeping alone and together are conducted across diverse circumstances. . Results Still, routinely bedsharing infants more frequently faced straight ahead compared with routinely solitary sleeping infants on the solitary night. For example, the RB group on the SN faced up for 20% percent of their sleep period time, while the solitary sleeping infants, on average, faced up for only 6.4 % of their time in bed. The percentage range of their sleep period time sleeping alone in which infants looked to their left was for 26.6% (range 0-52%) of the night, to the right 68.6%, (range 34-100) and facing up about 4.8% (range 0-14%). Routine bedsharing infants, while sleeping alone, looked to the left for an average of 20.7% of the night (range 3.5-51%), to the right 58.7% (range 19-74%) and looked straight ahead 20.6% (range 0-74 %). The mothers’ presence or absence in bed with her infant determines the direction in which infants orient their face for most of the night, regardless of whether or not at home they routinely bedshare or sleep alone. As Figures 1- 4 illustrate, for routinely bedsharing and solitary sleeping infants on the bedsharing night in the lab, infants faced in the direction of their mothers’ bodies for 98.3% (sd 3.1) and 96.4% (sd 7.5) of the night respectively. On solitary sleeping nights, regardless of routine sleeping arrangements at home, infants from both groups moved their heads more frequently from one direction to another (right, left, and/or up) compared to the bedsharing night. No significant predominant orientation occurred, although in most cases, babies avoided the “face up position.” The importance of detailed investigations into the nighttime interactions between mothers and infants is especially critical at this time, given the sweeping public health recommendations by the Consumer Product Safety Commission in the United States against any and all bedsharing. Moreover, breastfeeding episodes doubled when mother and their infants slept together in the same bed (Figure 5), although more infants from the routinely breast feeding-bedsharing subgroup received more feeds on average regardless of where the baby slept. The average number of breast feeds for the routinely bedsharing infant on both the bedsharing night and solitary night was 4.3 breast feeds and 2.3 breast feeding episodes, respectively. On their routine night in the lab, solitary sleeping infants, sleeping alone, on average received 1.4 breast feeding episodes, with three of these infants receiving one feed while two infants received two feeds. On the bedsharing night, however, one infant (number 3) from the routinely solitary sleeping group jumped from receiving only two feeds while sleeping alone to receiving 13 feeds when sleeping next to mother. This clearly skewed the number of breast feeds for the routinely solitary sleeping group on the bedsharing night, with a mean of 5 breast feeds (range 1-13). On their bedsharing night, routinely bedsharing infants per breast feeding episode breast fed for an average of 7.7 minutes, with a total nightly average of breast feeding, per infant, of 31.9 minutes. This compared with a mean duration per episode of breast feeding for routinely solitary sleeping infants on their bedsharing night of 10.1 minutes, with a nightly average of breast feeding per infant in this group of 41.4 minutes. On the solitary night, routinely bedsharing infants on average breast fed per episode for 7.9 minutes (range 5.5-11.5 minutes), compared with an average breast feeding episode of 14.4 minutes (range 6-20) and an average of 10.3 total minutes of nightly breast feeding per infant for the routinely solitary sleeping infants (range 6-18 minutes). (See figures 6 and 7). Methods Twelve mother-infant pairs (24 mothers and infants) were studied and are divided between seven dyads who routinely bedshared (RB) from birth and 5 who routinely slept solitarily (RS). Routine bedsharing infants, the RB sub-group, were defined as bedsharing with the mother for at least 4 hours per night, 5 days per week; the routinely solitary sleeping infants (RS) were defined as bedsharing no more than 1 night per week for any part of the night. Subjects were recruited from the Birthing Center at the University of California Irvine Medical Center. The protocol was approved by the University’s Human Subjects Review Committee. All mothers were Latina because bedsharing is an accepted practice in this ethnic group. Inclusion criteria for infants were that they were 11-15 weeks old at the time of the sleep studies; were in good health, with normal growth and development; weight >2,500 g and had been >37 weeks of gestational age at delivery; had a 5-minute Apgar score > 8; had no history of SIDS in first-degree relatives; and had no history of prolonged apnea or an ALTE (5). Sleep studies were performed in the University Medical Center Sleep Disorders Center, a facility accredited by the American Sleep Disorders Association. Mother-infant pairs underwent three consecutive nights of polysomnography (see picture below). There was an initial adaptation night, matching the routine home sleeping arrangement, followed by a bedsharing night (BN) and a solitary sleeping night (SN) in randomly assigned order. For solitary sleeping, infants were placed in a standard crib in a room adjacent to that of the mother, with the doors between them ajar. On the bedsharing night(s), mother-infant pairs shared the same twin-size bed used by the mothers for solitary sleeping. Infants were maintained on their usual breast feeding and sleeping schedules, with mothers performing all caretaker interventions ad libitum. Breast feeding behavior was quantified as breast feeding episodes. A breast feeding episode began and ended with the infant latching on to the breast and detaching, respectively, but also included very short interruptions during which the mother switched from one breast to the other. These interruptions were a number of seconds and were below 1-minute resolution of the digital clock. A new breast feeding episode was scored if breastfeeding was interrupted by maternal behaviors that indicated an apparent attempt by the mother to terminate feeding (i.e. by closing her bra or night gown, attempting to leave the room, or by attempting to return to sleep) (6). On the solitary night, babies were scored for three possible facial orientations: facing right, left or up. On the bedsharing night, facial orientation was scored when babies either faced toward mothers, or faced to the opposite side. (While sleeping with mothers, infants rarely, if at all, looked straight up so this descriptor was dropped on the BN). Nothing an infant needs, or can or cannot do, makes sense except in light of the mother’s body Research funded by National Institutes of Child Health and Human Development RO1 27482 Discussion and Conclusion The most important and significant finding in this study is that when mothers sleep in proximity, their infant’s behavior changes in many ways, having potentially important implications for both maternal and infant health. Whether routinely bedsharing or not, all infants responded to their mothers presence in bed by orienting their face in her direction. In all bedsharing night instances (except for two infants) compared to the nights in the laboratory in which they slept in a separate room, both routinely bedsharing and routinely solitary sleeping infants often doubled, tripled and sometimes quadrupled the number of their breast feeding episodes. Previous to this study, McKenna et. al showed amongst this same subject population that a variety of sensory modalities, such as touch, sound, and mutual movements, act in concert amongst bedsharing mother-baby dyads to significantly change sleep architecture, arousal patterns, sleep positions, body temperature, hear rate and total amount of nighttime infant crying behavior, as well as the duration of both maternal and infant sleep (1). It is clear, then, similar to Hofer’s perspective, mothers’ bodies can and often do act as hidden regulators of their infant’s physiology (7). That is, our overall findings are consistent with the mechanisms described by Cernoch and MacFarlane (8, 9): they demonstrate that by two weeks of age, breast fed infants preferentially orient (by head turning) toward odors from their mothers’ breasts and axillary regions during sleep as well as waking (8). Infants in our sample not only slept in a different orientation compared with when they slept alone, but it seems likely that proximity to mothers breast milk odors, and /or her movements which induce more arousals and lighter sleep in her infant also explains why babies breast feed so much more in the bedsharing environment (1). Overall, sleeping close to the mother creates a sort of sensory bridge that induces related responses, we speculate, of increased breast feeding behavior preceded by intense and almost continuous sensory attention given to the mother by the infant, who sleeps by turning toward her. The most important and significant finding in this study is that when mothers sleep in proximity, their infant’s behavior changes in many ways, having potentially important implications for both maternal and infant health. References 1. McKenna, J. J., and Mosko, S. (2001). Mother-infant cosleeping: Toward a new scientific beginning. In Sudden Infant Death Syndrome: Problems, Puzzles, Possibilities, ed. R. Byard and H. Krous. New York: Arnold Publishing. 2. Scheers, N. J., Rutherford, G.W., and Kemp, J.S. (2003). Where should infants sleep? A comparison of risk for suffocation of infants sleeping in cribs, adult beds, and other sleeping locations. Pediatrics. 112(4): 883-889. 3. Drago DA, Dannenberg AL. Infant mechanical suffocation deaths in the United States, 1980-1997. Pediatrics 1999; 103:59. 4. McKenna, J. J. Thoman, E., Anders, T., Sadeh, A., Schechtman, V., and Glotzbach, S. (1993). Infant-parent co-sleeping in evolutionary perspective: Implications for understanding infant sleep development and the Sudden Infant Death Syndrome (SIDS). Sleep. 16(3): 263-282. 5. Mosko, S, McKenna JJ, Drummond, S. Infant Sleep Architecture During Bedsharing and Possible Implications for SIDS. Sleep and Pediatrics. 1996; 19(9):677-684. 6. McKenna, J. J. et al. (1997). Bed sharing promotes breastfeeding. Pediatrics. 100: 214-219. 7. Hofer MA. Hidden regulatory processes in early social relationships. In: Bateson PPG, Klopfer PH, eds. Perspectives in Ethology, Vol. 1. New York: Plenum 1978:136-66. 8. Cernoch JM, Porter RH. Recognition of maternal axillary odors by infants. Child Dev. 1985; 56:1593-1598. 9. MacFarlane AJ. Olfaction in the development of social preferences in the human neonate. Parent infant interaction. Ciba Found Symp. 1975; 33:103-113.






