Download
1 / 1
10 likes | 222 Views
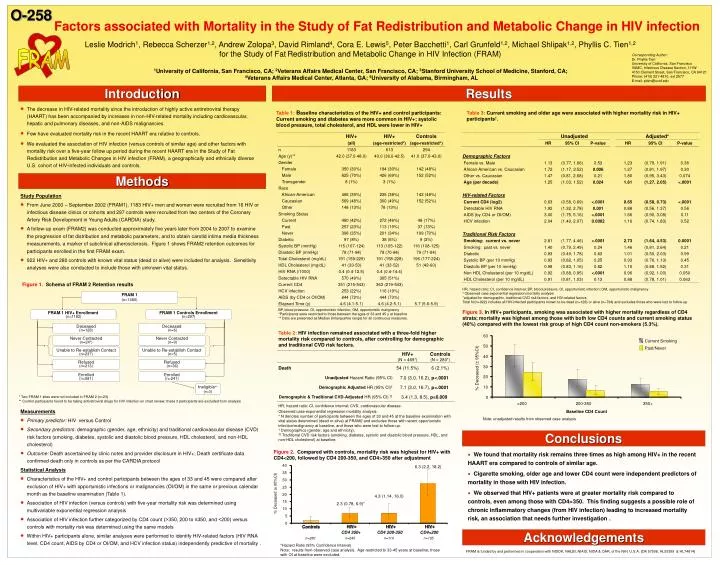
FRAM. Figure 1. Schema of FRAM 2 Retention results. 60. Current Smoking. 50. Past/Never. 40. 30. % Deceased (± 95%CI). 20. 10. * Two FRAM 1 sites were not included in FRAM 2 (n=23)

E N D
FRAM Figure 1. Schema of FRAM 2 Retention results 60 Current Smoking 50 Past/Never 40 30 % Deceased (± 95%CI) 20 10 * Two FRAM 1 sites were not included in FRAM 2 (n=23) ** Control participants found to be taking antiretroviral drugs for HIV infection on chart review; these 3 participants are excluded from analysis 0 <200 200-350 350+ Baseline CD4 Count FRAM 1 (n=1480) FRAM 1 HIV+ Enrollment (n=1183) FRAM 1 Controls Enrollment (n=297) 40 6.3 (2.2, 18.2) 35 Deceased (n=128) Deceased (n=6) 30 25 Never Contacted (n=24*) Never Contacted (n=9) % Deceased (± 95%CI) 20 4.3 (1.14, 16.0) Unable to Re-establish Contact (n=237) Unable to Re-establish Contact (n=5) 15 2.3 (0.78, 6.9)* 10 Refused (n=213) Refused (n=36) 5 0 Enrolled (n=581) Enrolled (n=241) HIV+ HIV+ HIV+ Controls CD4 350+ CD4 200-350 CD4<200 Ineligible** (n=3) n=280 n=245 n=114 n=105 *Hazard Ratio (95% Confidence Interval) Note: results from observed case analysis. Age restricted to 33-45 years at baseline; those with OI at baseline were excluded. O-258 Factors associated with Mortality in the Study of Fat Redistribution and Metabolic Change in HIV infection Leslie Modrich1, Rebecca Scherzer1,2, Andrew Zolopa3, David Rimland4, Cora E. Lewis5, Peter Bacchetti1, Carl Grunfeld1,2, Michael Shlipak1,2, Phyllis C. Tien1,2 for the Study of FatRedistribution and Metabolic Change in HIV Infection (FRAM) Corresponding Author: Dr. Phyllis Tien University of California, San Francisco VAMC, Infectious Disease Section, 111W 4150 Clement Street, San Francisco, CA 94121 Phone: (415) 221-4810, ext 2577 E-mail: ptien@ucsf.edu 1University of California, San Francisco, CA; 2Veterans Affairs Medical Center, San Francisco, CA; 3Stanford University School of Medicine, Stanford, CA;4Veterans Affairs Medical Center, Atlanta, GA; 5University of Alabama, Birmingham, AL Introduction Results • The decrease in HIV-related mortality since the introduction of highly active antiretroviral therapy (HAART) has been accompanied by increases in non-HIV-related mortality including cardiovascular, hepatic and pulmonary diseases, and non-AIDS malignancies. • Few have evaluated mortality risk in the recent HAART era relative to controls. • We evaluated the association of HIV infection (versus controls of similar age) and other factors with mortality risk over a five-year follow up period during the recent HAART era in the Study of Fat Redistribution and Metabolic Changes in HIV infection (FRAM), a geographically and ethnically diverse U.S. cohort of HIV-infected individuals and controls. Table 1:Baseline characteristics of the HIV+ and control participants: Current smoking and diabetes were more common in HIV+; systolic blood pressure, total cholesterol, and HDL were lower in HIV+ Table 3: Current smoking and older age were associated with higher mortality risk in HIV+ participants†. Methods Study Population • From June 2000 – September 2002 (FRAM1), 1183 HIV+ men and women were recruited from 16 HIV or infectious disease clinics or cohorts and 297 controls were recruited from two centers of the Coronary Artery Risk Development in Young Adults (CARDIA) study. • A follow-up exam (FRAM2) was conducted approximately five years later from 2004 to 2007 to examine the progression of fat distribution and metabolic parameters, and to obtain carotid intima media thickness measurements, a marker of subclinical atherosclerosis. Figure 1 shows FRAM2 retention outcomes for participants enrolled in the first FRAM exam. • 922 HIV+ and 280 controls with known vital status (dead or alive) were included for analysis. Sensitivity analyses were also conducted to include those with unknown vital status. Measurements • Primary predictor: HIV versus Control • Secondary predictors: demographic (gender, age, ethnicity) and traditional cardiovascular disease (CVD) risk factors (smoking, diabetes, systolic and diastolic blood pressure, HDL cholesterol, and non-HDL cholesterol) • Outcome: Death ascertained by clinic notes and provider disclosure in HIV+; Death certificate data confirmed death only in controls as per the CARDIA protocol Statistical Analysis • Characteristics of the HIV+ and control participants between the ages of 33 and 45 were compared after exclusion of HIV+ with opportunistic infections or malignancies (OI/OM) in the same or previous calendar month as the baseline examination (Table 1). • Association of HIV infection (versus controls) with five-year mortality risk was determined using multivariable exponential regression analysis • Association of HIV infection further categorized by CD4 count (>350, 200 to ≤350, and <200) versus controls with mortality risk was determined using the same models • Within HIV+ participants alone, similar analyses were performed to identify HIV-related factors (HIV RNA level, CD4 count, AIDS by CD4 or OI/OM, and HCV infection status) independently predictive of mortality . Figure 3. In HIV+ participants, smoking was associated with higher mortality regardless of CD4 strata; mortality was highest among those with both low CD4 counts and current smoking status (40%) compared with the lowest risk group of high CD4 count non-smokers (5.3%). Table 2:HIV infection remained associated with a three-fold higher mortality risk compared to controls, after controlling for demographic and traditional CVD risk factors. Note: unadjusted results from observed case analysis Conclusions Figure 2. Compared with controls, mortality risk was highest for HIV+ with CD4<200, followed by CD4 200-350, and CD4>350 after adjustment • We found that mortality risk remains three times as high among HIV+ in the recent HAART era compared to controls of similar age. • Cigarette smoking, older age and lower CD4 count were independent predictors of mortality in those with HIV infection. • We observed that HIV+ patients were at greater mortality risk compared to controls, even among those with CD4>350. This finding suggests a possible role of chronic inflammatory changes (from HIV infection) leading to increased mortality risk, an association that needs further investigation . Acknowledgements FRAM is funded by and performed in cooperation with NIDDK, NHLBI, NIAID, NIDA & OAR, of the NIH, U.S.A. (DK 57508, HL53359 & HL74814)

![FERROELECTRIC RAM [FRAM]](https://cdn1.slideserve.com/1817127/ferroelectric-ram-fram-dt.jpg)