Download
1 / 5
50 likes | 189 Views
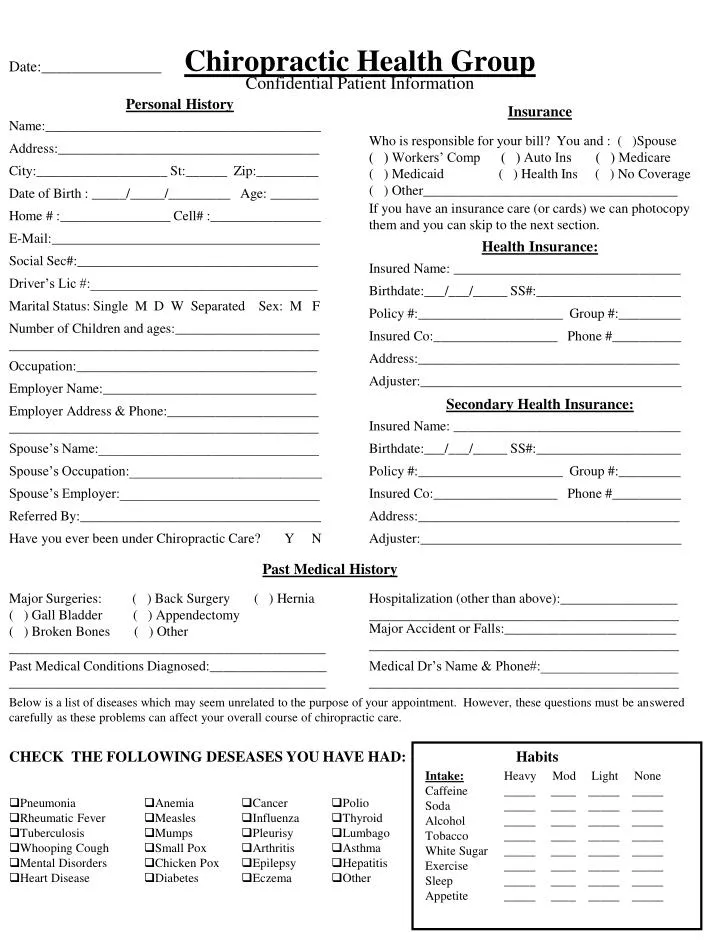
Habits. Intake: Caffeine Soda Alcohol Tobacco White Sugar Exercise Sleep Appetite. Heavy Mod Light None _____ ____ _____ _____ _____ ____ _____ _____ _____ ____ _____ _____ _____ ____ _____ _____

E N D
Habits Intake: Caffeine Soda Alcohol Tobacco White Sugar Exercise Sleep Appetite Heavy Mod Light None _____ ____ _____ _____ _____ ____ _____ _____ _____ ____ _____ _____ _____ ____ _____ _____ _____ ____ _____ _____ _____ ____ _____ _____ _____ ____ _____ _____ _____ ____ _____ _____ Date:________________ Confidential Patient Information Personal History Insurance Name:________________________________________ Who is responsible for your bill? You and : ( )Spouse ( ) Workers’ Comp ( ) Auto Ins ( ) Medicare ( ) Medicaid ( ) Health Ins ( ) No Coverage ( ) Other_____________________________________ Address:______________________________________ City:___________________ St:______ Zip:_________ Date of Birth : _____/_____/_________ Age: _______ If you have an insurance care (or cards) we can photocopy them and you can skip to the next section. Home # :________________ Cell# :________________ E-Mail:_______________________________________ Health Insurance: Social Sec#:___________________________________ Insured Name: _________________________________ Driver’s Lic #:_________________________________ Birthdate:___/___/_____ SS#:_____________________ Marital Status: Single M D W Separated Sex: M F Chiropractic Health Group Policy #:_____________________ Group #:_________ Number of Children and ages:_____________________ _____________________________________________ Insured Co:__________________ Phone #__________ Address:______________________________________ Occupation:___________________________________ Adjuster:______________________________________ Employer Name:_______________________________ Secondary Health Insurance: Employer Address & Phone:______________________ _____________________________________________ Insured Name: _________________________________ Spouse’s Name:________________________________ Birthdate:___/___/_____ SS#:_____________________ Spouse’s Occupation:____________________________ Policy #:_____________________ Group #:_________ Spouse’s Employer:_____________________________ Insured Co:__________________ Phone #__________ Referred By:___________________________________ Address:______________________________________ Have you ever been under Chiropractic Care? Y N Adjuster:______________________________________ Past Medical History Major Surgeries: ( ) Back Surgery ( ) Hernia ( ) Gall Bladder ( ) Appendectomy ( ) Broken Bones ( ) Other ______________________________________________ Hospitalization (other than above):_________________ _____________________________________________ Major Accident or Falls:_________________________ _____________________________________________ Past Medical Conditions Diagnosed:_________________ ______________________________________________ Medical Dr’s Name & Phone#:____________________ _____________________________________________ Below is a list of diseases which may seem unrelated to the purpose of your appointment. However, these questions must be answered carefully as these problems can affect your overall course of chiropractic care. CHECK THE FOLLOWING DESEASES YOU HAVE HAD: • Pneumonia • Rheumatic Fever • Tuberculosis • Whooping Cough • Mental Disorders • Heart Disease • Anemia • Measles • Mumps • Small Pox • Chicken Pox • Diabetes • Cancer • Influenza • Pleurisy • Arthritis • Epilepsy • Eczema • Polio • Thyroid • Lumbago • Asthma • Hepatitis • Other
CHECK ANY OF THE FOLLOWING YOU HAVE HAD WITHIN THE LAST 6 MONTHS • Musculo-Skeletal • Low Back Pain • Pain Between Shoulders • Neck Pain • Arm Pain R L • Leg Pain R L • Joint Pain/Stiffness • Walking Problems • Jaw Pain / Clicking • General Stiffness Nervous System • Nervous • Numbness • Paralysis • Dizziness • Forgetfulness • Confusion/Depression • Fainting • Convulsions • Cold/Tingling Extremities • Stress Genito-Urinary • Bladder Trouble • Painful/Excessive Urination • Discolored Urine • Gastro-Intestinal • Poor/Excessive Appetite • Excessive Thirst • Frequent nausea • Vomiting • Diarrhea • Constipation • Hemorrhoids • Liver Problems • Gall Bladder Problems • Weight Trouble • Abdominal Cramps • Gas/Bloating • Heartburn • Black/Bloody Stool • Colitis Vascular • Stroke • Chest pain • Shortness of Breath • Irregular Heartbeat • Heart Problems • Blood Pressure • Lung / Congestion • Varicose Veins • Ankle Swelling • EENT • Vision Problems • Dental Problems • Sore Throat • Ear Aches • Hearing Difficulty • Stuffed Nose General • Fatigue • Allergies • Loss of Sleep • Fever • Headaches Family History The following members have the same or similar problem as I do: • Mother • Father • Brother / Sister • Spouse • Child • Male/Female • Menstrual Irregularity • Menstrual Cramps • Vaginal Pain/Infection • Breast Pain/Lumps • Prostrate Enlargement • Sexual Dysfunction • Other: ___________________________________________________________________________ Females Only When was your last period?_______________ Are you Pregnant? Y N Not Sure Current Health Condition Purpose of this Appointment:______________________ ______________________________________________ Activities that are painful to perform: ( ) Sitting ( ) Standing ( ) Walking ( ) Bending ( ) Lying Down ( ) Running Date Symptoms Appeared: _____/_____/___________ Drugs you now take: _____________________________________________ _____________________________________________ Have you ever had the same or similar condition? Y N If yes, when:___________________________________ How often is the pain? ( ) Constant ( ) Comes & Goes Other_________________________________________ Have you seen another doctor for this condition: Y N If yes, Name & Address of Dr:____________________ _____________________________________________ Is this condition getting progressively worse: Y N This condition is interfering with: ( ) Work ( ) Sleep ( ) Daily Routine ( ) Other:_____________________ What type of treatment did you receive?______________________________________ _____________________________________________ Do you suffer from any condition other than that which you are now consulting us: Y N If Yes , Please Describe: _____________________________________________ _____________________________________________ What aggravates the condition (makes it worse)? ______________________________________________ ______________________________________________
Describe how it feels: ( ) Numb ( ) Aching ( ) Dull ( ) Tingling ( ) Throbbing ( ) Stiffness ( ) Sharp ( ) Cramping ( ) Burning Please mark the area(s) of injury and type of discomfort (letters) as shown in the example below. N = Numbness T = Tingling A = Aching B = Burning S = Stabbing D = Dull Please rate your pain on the scale below. 0 = No Pain and 10 = Severe Pain 1 2 3 4 5 6 7 8 9 10 1 2 3 4 5 6 7 8 9 10 1 2 3 4 5 6 7 8 9 10 Pain Currently Pain at its worst Pain typically I understand and agree that health and accident insurance policies are an agreement between an insurance carrier and myself. I acknowledge full responsibility for payment of services and agree to pay them in full at the time of service, unless other arrangements are made in advance. Furthermore, I understand that this chiropractic office will prepare any necessary reports and forms to assist me in making collections from the insurance company and that any amount authorized to be paid directly to this chiropractic office will be credited to my account on receipt. I also give this office power of attorney to endorse checks made out to me, to be credited to my account. However, I clearly understand and agree that all services rendered me are charged directly to me and that I am personally responsible for payment. I also understand that if I suspend or terminate my care and treatment, any fees for professional services rendered me will be immediately due and payable. In addition, I will pay all collection agency and/or attorney’s fees of 1/3 of the outstanding balance plus court costs, if my account is ever referred to same. The X-ray negatives will remain the property of this office, being on file where they may be seen at any time with a patient of this office. The Doctor will not be held responsible for any pre-existing medically diagnosed or undiagnosed conditions, nor for any medical diagnosis. Patient Signature:_____________________________________________________ Date:____________________ Guardian Signature Authorizing Care:_____________________________________ Date:____________________
HIPPA Declaration • The Practice: • Is required by federal law to maintain the privacy of your Protected Health Information (PHI) and to provide you with this Privacy Notice detailing the Practice’s legal duties and privacy practices with respect to your PHI • Under the Privacy Rule, may be required by State Law to grant greater access or maintain greater restrictions on the use or release of your PHI than that which is provided for under federal law • Is required to abide by the terms of the Privacy Notice • Reserves the right to change the terms of this Privacy Notice and to make the new Privacy Notice provisions effective for all your PHI that it maintains • Will distribute any revised Privacy Notice to you prior to implementation • Will not retaliate against you for filing a complaint • EFFECTIVE DATE • This Notice is in effect as of 11/30/2012 • PATIENT ACKNOWLEDGEMENT • By subscribing my name below, I acknowledge receipt of this notice, and my understanding and my agreement to its terms. • ___________________________ • PATIENT • ___________________________ • DATE • FOR PRACTICE USE ONLY • Practice Documentation of Good Faith Effort to Obtain Acknowledgement • Patient’s acknowledgement of this notice could not be obtained because • ____ Patient refused to sign • ____Communication barrier prohibited obtaining acknowledgement • ____Emergency circumstances • ____Other • Details: • ____________________________ • Signature of Practice • ____________________________ • Date
CONSENT TO TREATMENT • Health care providers are required to advise patients of the nature of the treatment to be provided, the risks and benefits of the treatment, and any alternatives to the treatment. • There are some risks that may be associated with treatment, in particular you should note: • a. ‘While rare, some patients have experienced rib fractures or muscle and ligament sprains or strains following treatment; • b. There have been rare reported cases of disc injuries following cervical and lumbar spinal • adjustment although no scientific study has ever demonstrated such injuries are caused, or maybe caused, by spinal or soft tissue manipulation or treatment. • c. There have been reported cases of injury to a vertebral artery following osseous spinal • manipulation. Vertebral artery injuries have been known to cause a stroke, sometimes withserious neurological impairment, and may, on rare occasion, result in paralysis or death. The possibility of such injuries resulting from cervical spine manipulation is extremely remote; • Osseous and soft tissue manipulation has been the subject of government reports and multi-disciplinary studies conducted over many years and have demonstrated it to be highly effective treatment of spinal conditions including general pain and loss of mobility, headaches and other related symptoms. Musculoskeletal care contributes to your overall well being. The risk of injuries or complications from treatment is substantially lower than that associated with many medical or other treatments, medications, and procedures given for the same symptoms. • I acknowledge I have discussed the following with my healthcare provider: • a. The condition that the treatment is to address; • b. The nature of the treatment; • c. The risks and benefits of that treatment; and • Any alternatives to that treatment. • I have had the opportunity to ask questions and receive answers regarding the treatment. • I consent to the treatments offered or recommended to me by my healthcare provider, including osseous and soft tissue manipulation. I intend this consent to apply to all my present and future care with ___________________________________ (health care providers name). • Dated this ___________ day of _____________ 20___ • ______________________________ _______________________________ • Patient signature (or Legal Guardian) Signature of Witness • Print Name:_____________________ Print Name:_____________________