Download
1 / 58
650 likes | 902 Views
Robotics and Ablation The Erasmus MC experience. Tamas Szili-Török MD, PhD Erasmus MC - Rotterdam. Sensei. MNS-Stereotaxis. Robotics. Karel Capek- 1920: R.U.R (Rossum Universal Robots) Labor- Robota (work) Asimov: robotics- the scientific field studying robots. ROBOTICS:

E N D
Robotics and AblationThe Erasmus MC experience Tamas Szili-Török MD, PhD Erasmus MC - Rotterdam
Sensei MNS-Stereotaxis
Robotics Karel Capek- 1920: R.U.R (Rossum Universal Robots) Labor- Robota (work) Asimov: robotics- the scientific field studying robots
ROBOTICS: Definition of the “robot”: A robot is a virtual or mechanical arteficial agent, which is able to do tasks on its own.
Sensei MNS-Stereotaxis
Imrpovement of electrophysiology procedures Efficacy Efficiency Reproducibility Safety
Ways to achieve standardization of EP procedures • Simplification • Automation • Integration
What is magnetic navigation? • Magnetic Navigation is an interaction between: • External magnetic field of a specified direction and magnitude • Tiny magnet in the tip of the endovascular device End result is ALIGNMENT of the tip magnet with the field direction There is NO significant magnetic pull, push, attract, or repel effect on the endovascular device
What is magnetic navigation? • Two remotely controlled magnets move changing the orientation of the magnetic field in any direction. • A small magnet located in the tip of the catheter orients itself to the remotely determined magnetic field.
Magnetic Navigation System Theoretical advantages: • Atraumatic, flexible catheter design • Unrestricted catheter navigation • Reproducibility using stored magnetic vectors • Enhanced stability • Less fluoroscopy exposure both for the patient and for the operator
Optimizing RF power delivery • Appropriate therapy + tip delivery= clinical success
Patients • 610 patients underwent EP and ablation using either MNS or MAN • MNS group: 292 pts • MAN group: 318 pts
Subgroup analysis Based on the diagnosed arrhythmia: AFib, AFl/AT, AVJ, AVNRT, CMT and VT The VT subgroup was further divided to structural heart disease associated (VT-SHD) or non-structural heart disease associated (VT-NSHD) VTs
Data collection and analysis • Acute success rate • Recurrence during FU (3 month following the procedure, and every 3 month thereafter except for AVNRT, AFl, AVJ and CMT) • Fluoroscopy and procedure times • Complications
Complications • Major: • stroke • death • pericardial effusion or tamponade • major bleeding • permanent AV block • Minor: • minor bleeding • temporary AV block
MNS MAN p < 0,05 Acute Success Rate Recurrence Rate Results Acute Success and Recurrence
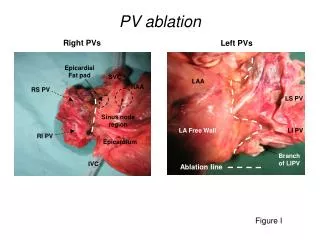
Ablation of atrial flutter 61 patients were divided to 3 groups 24 patients were treated with 8 mm tip catheter using manual navigation technique (MAN) 18 patients were treated with 8 mm tip catheter using MNS (MNS-8mm) 19 patients were treated with irrigated tip catheter using MNS (MNS-irr)
Endpoints Primary: success within 15 applications Secondary: procedure time, fluoroscopy time
Results: MVGT- MNS registry 61 pts included MNS 37 pts Manual Navig. 8 mm tip 24 pts MNS - irr 19 pts MNS - 8 mm 18 pts Success within 15 application 18 pts Success within 15 application 20 pts Max of 15 RF application failure 1+6+4 = 11 pts Success within 15 application 12 pts Open irrigation tip catheter
Acute Success Rates Bidirection isthmus block was achieved within 15 applications: MAN: 20/24=83% MNS – 8mm: 12/18=67% MNS – irrigation tip: 18/19=95% Isthmus block could be reached in all cases after switching to manual-guided irrigation tip catheters. p<0.05
Complications II. (group MNS) Probably no any reason to use 8 mm MNS catheter
Ablation of ventricular tachycardias SHD: structural heart disease
Results: Acute success rate SHD: structural heart disease
Recommendations • Left atrium: 3,5 mm tip electrode, open irrigation, posterior wall: 30 W, max power: 45 W (only at the ridge between LSPV and appendage, in case of more segmental RF applications: reduce to 20-25 W, irr: 17 ml • Left ventricle: min. 50 W for the ventricle. Irrigation starts at 20 ml, if power goes to 55 W irr: 30 ml/min • In standard WPW procedures, 4 mm tip standard electrode, 55 W power, 60 °C • In CTI dependant flutter: maximum voltage guided technique, 3.5 mm tip irrigation catheter, min 55 W power level- but high irrigation level starting at 30 ml (steam pop). preferably ½ 6 (more septal) • In AVNRT, 4 mm tip standard catheter, power titration from 10 W up to 40-50 W, 50 °C • RV: Irrigation tip, starting with relatively low irr. level (10 ml), power 45 W
The effect on ablation results of improved catheter and mapping technology Triedman et al, JACC, 2002 37
Consequences of high catheter contact force Tilz et al, JCE, 2010
Magnetic catheters provide constant contact 50 Watts, 60 seconds 25 Watts, 60 seconds Cross-sections show full thickness lesions in 5mm thick tissue Epicardial view of endocardially-delivered lesions in a canine model
History • 1991 Anterior and apical MI, conservative therapy • 1992 CABG (venous grafts LAD, MO, RDP) • 2000 Monomorphic VT, VT ablation (other center) and amiodarone therapy. • 2002 Multiple hospitalization, heart failure due to ischemic origin DCM • 2003 Polymorph VTs, CAG: no stenosis of the grafts, EF 25%, DDD ICD impl.
History • 2006 Repositioning of the ICD due to decubitus • 2007 Multiple ICD shocks for VF. • 2008 Polymorph VTs, ICD shocks. EF 26%.CAG: Occluded native coronaries (RCA, LAD, LCX). Intact venous grafts. VT-ablation (postero-lateral and apical applications). • 2008 Recurrant slow-VTs. Amiodarone+lidocaine (oral mexiletine started) • 2009 Recurrant VTs, multiple shocks, long-term hospitalization. Heart-transplant waiting list. • 2010.02. Recurrant VTs again