Download
1 / 43
430 likes | 490 Views
This educational resource covers the basics of gallbladder disease, including types of gallstones, acute cholecystitis workup, medical vs. surgical management, ascending cholangitis, and more. Explore anatomy, physiology, pathologies, and treatment options with expert insights.

E N D
Gallbladder Disease Gazi Rashid Lindsey Urquia
5 Takeaways • Basic HPB layout and 2 important views during surgery • Different types of gallstones and their risk factors • Walk through an H&P & workup for acute cholecystitis • Basics of Medical vs. Surgical mgmt for acute cholecystitis • Presentation and acute management of ascending cholangitis Extra: Recognize • Basic presentation & pathophys of gallstone ileus • Imaging & management of Porcelain GB • Surgical indications for asymptomatic cholelithiasis
Anatomy : Gazi - 5 min • Minor: Symp Chole, Choledocho, • Physiology/types of GS/risk factors: Lindsey - 5 min • GB pathology • Acute chole: Lindsey - 15 min • Patho → Pres • DDx • W/U – Labs, Imaging • Medical • Operative • Ascending chol : Gazi - 10 min • Patho → Pres (Triad, Pentad) • W/U → labs, imaging • Med/ICU mgmt • Operative/ERCP • Cases – core info (x3) - 10 min (6, 4) - I don’t know that we’ll have time to do 3 cases • Biliary colic-– Lindsey/Gazi + counseling • Acute Chole - 1 liner→ diagnosis: history/PE/labs/US/management - 5 Qs each - maybe include the “Pearls” here • Asc Chol - 5 review Qs, as this isn’t a typical H&P • Misc - Porcelain GB, Gallstone Ileus (5 min) • “pearls”– • Time for questions - 10-15 min (mention oral exams, resources to learn rest of biliary dz) • Appendix - at their own pleasure
Anatomy Draw the hepatobiliary system - gallbladder, liver, pancreas, duodenum, and what connect them
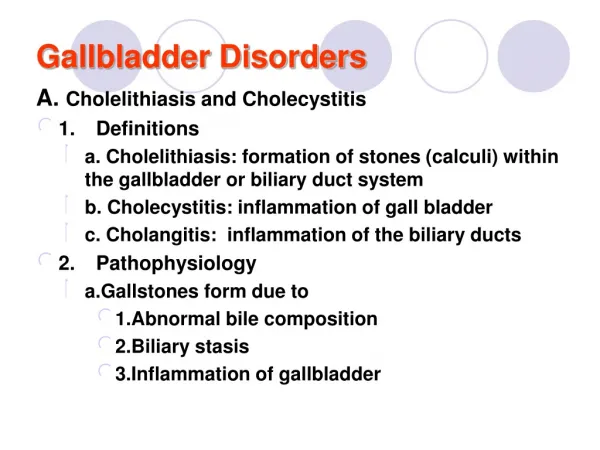
Gallbladder • Cholelithiasis • Asymp. Vs Symp • Calculous Cholecystitis • Porcelain GB • Gallstone Ileus • Acalculous Cholecystitis • Gangrenous Cholecystitis • GB Carcinoma CDB - Choledocholithiasis - Ascending Cholangitis - Cholangiocarcinoma - Strictures from ERCP Cystic Duct - Mirizzi Syndrome Sphincter of Oddi Biliary Dyskinesia Cancer at the Head of the Pancreas
Critical View of Safety
Types of gallstones/risk factors • Biliary sludge – cholesterol crystals, Ca bilirubinate granules & mucin maxtrix • Impaired/slow contractility or bile stasis • Cholesterol (70-80%) • Most common • Increased ratio of chol:salts • Hormone (preg, OCP) • Pigmented (20-30%) • Bilirubin & calcium salts (20% cholesterol) • Cirrhosis, hemolytic anemia, hereditary spherocytosis
Acute cholecystitis • Pain – unrelenting right upper quadrant, midepigastric pain • Vs. Biliary colic • Nausea & vomiting • Fever/chills • Labs * - elevated enzymes/Br but relatively low • Obstruction of cyst duct from gallstone • 95% - calculi • 5% - acalculous (sludge) • GB continues to produce mucous ➔ distension ➔ venous congestion inflamed, edematous wall ➔ arterial inflow impaired ➔ stone dislodges (ischemia 5-10%)
Normal Gallbladder imaging
Acute Cholecystitis imaging
Acute Cholecystitis imaging
HIDA Scan(Hepatobiliary Iminodiacetic acid) If there’s a question…get a HIDA Highly sensitive & specific! (95%) imaging
Acute Cholecystitis imaging
Acute Cholecystitis medical mang • NPO • IV fluids • IV antibiotics • E. Coli, Klebsiella, Enterobacter, Bacteroides, Clostridium coverage • 2nd gen cephalosporin (cefoxitin) • Fluoroquinolones (Ciprofloxacin, Levofloxacin) • Ampicillin-sulbactam (Unasyn) • Surgery! treatment
Cholecystectomy • NPO, IVF, IV abx • Classic: Surgery safe if within 72 hours • Identify anatomical views & critical view • Intraoperative cholangiogram (IOC) – high suspicion for CBD stone • Lap > open conversion rate 0-20% treatment
Cholecystectomy treatment
Ascending cholangitis • Terms: Choledocholithiasis vs. Ascending Cholangitis • Acute Presentation (Charcot’s Triad): • Jaundice, RUQ pain, Fever • Complicated by Reynold’s pentad: Triad + Hypotension + AMS (Septic shock) • Not always due to stones!
Workup • Leukocytosis • Cholestatic Pattern of Liver Injury • ALP, GGT, Bilirubin >>> AST, ALT • All can be elevated • RUQ U/S: • Stone not always seen • Look for CBD dilatation
Management of Ascending Cholangitis • Mild ←→ Emergency! • Unstable patients: aggressive medical management, ICU • BP control:fluids, fluids, fluids • Monitoring • Blood cultures • Treatment: • IV broad spectrum antibiotics • Biliary decompression with ERCP (1st line) • Cholecystectomy when stable
Porcelain Gallbladder imaging
Gallstone Ileus • Misnomer! • Mechanical obstruction • Large impacted stone → Ischemia & pressure necrosis → Erosion into intestines→ cholecystic-enteric fistula • Bowel obstruction when stone is stuck at ileo-cecal valve
Gallstone Ileus Presentation • Elderly women with hx of biliary disease • Small bowel obstruction symptoms • N/V, diffuse abd pain, obstipation Imaging(plain films, CT scan) • Bowel obstruction findings: Air-fluid levels • Pneumobilia (gas in biliary tree) • Ectopic large gallstone
Case 1 42 y/o woman presents to clinic with abdominal pain 1. History – LOCATES 2. Physical exam 3. DDx 4. Labs 5. Management Bonus: What if this patient was asymptomatic and found – when would you do a cholecystectomy?
Case 1 • 42 y/o female with a 2 day history of RUQ & right upper back pain, assoc nausea. What’s your differential diagnosis? • Worse after meals. Similar episodes in the past. No f/c • Meds – OCP, MVI • PMH/PSH – HTN, hyperlipidemia, Lap gastric banding pathology
Acute Cholecystitis imaging
Diagnosis • History & physical exam • Ultrasound • 95% sensitive • Hyperechoic mobile densities within gallbladder with assoc hypoechoic shadowing diagnosis
Case 2 25 y/o female with a 2-day hx of fevers, chills, constant RUQ pain, scleral icterus, nausea, vomiting, BP 90/54, HR 117, T 39.1: • Next steps of management? • Other DDx? • Workup (Labs, Imaging, etc)? • What will 1st line imaging show? • What is the 1st-line therapeutic intervention? Describe it. Bonus: The pt.tells you that she’s had mouth sores & bloody diarrhea for months - what is the underlying pathology in this presentation?
Acute cholecystitis RUQ pain, nausea/vomiting, fever, increased WBC U/S (1st line): pericholecystic fluid, GB wall > 3mm thick, stones, sonographic Murphy’s HIDA 95% accurate Anatomy Modern Triangle of Calot: Cystic Artery, Hepatic Duct, Inf Liver Edge CVS: See cystic artery and cystic duct entering GB Acute cholangitis Charcot triad: (1) fever/chills + RUQ pain + jaundice Reynold’s pentad: Charcot’s triad + altered mental status + shock Emergency! Need ERCP summary
Symptomatic cholelithasis Intermittent RUQ pain, nausea, fever unlikely Diagnosis H&P, Ultrasound Gallstone Ileus 1 liner: Elderly women w/ SBO & history of biliary disease Transition point at ileocecal valve (stuck) Porcelain gallbladder Asymptomatic 25-50% assoc with gallbladder cancer summary
Case 2 • 79 y/o female with a 5 day history of diffuse abdominal pain, nausea, vomiting What’s your differential diagnosis? • Pain begin in RUQ, progressively worse, subjective chills • Meds – insulin, ASA • Pertinent hx – NH resident, diabetes pathology
Gallbladder Carcinoma • 0.5-1% of pop with cholelithiasis • Poor prognosis (unless T1a) • Most adenocarcinoma • Contracted (nondistended) • Risk Factors: adenomatous polyps, porcelain gallbladder (50%), biliary anomalies pathology
Gallbladder Carcinoma • Localized (lamina propria) • Cholecystectomy • Advanced Stage • radical cholecystectomy • Gallbladder + hepatic segments 4b & 5 + LND treatment
Mirrizzi Syndrome Common hepatic duct obstruction 2/2 impacted stone in cystic duct pathology
Biliary Dyskinesia • Impaired GB emptying or sphincter of Oddi relaxation • Biliary colic (post-prandial sharp RUQ pain), nausea • NO gallstones • Extensive w/u • HIDA + CCK • GB ejection fraction 35% or less pathology
Acalculous Cholecystitis • Seen in critically ill pt • Trauma • Burn • Prolonged TPN or NPO status (weeks) • Cardiopulmonary bypass • Often progress to gangrene or emphysematous cholecystitis • Fulminant course - has 40% mortality rate pathology
Imaging in Gallstone Ileus Imaging