Download

1 / 69
690 likes | 708 Views
Learn about acute CNS infection, etiology, bacterial pathogens, clinical features, diagnosis, and pathology of suppurative meningitis.

E N D
Suppurative Meningitis Yu Dan Department of Neurology West China Second University Hospital
conception Bacteria Virus Tuberculosis Fungus Parasite Spirochetal Pathogen CNS
Suppurative Meningitis • Acute infection of central nervous system(CNS). 90% of cases occur in the age of 1mo-5yr. • The inflammation of meninges caused by various bacteria. Common features in clinical practices include: fever, increased intracranial pressure, meningeal irritation. One of the most potentially serious infections, associated with high mortality (about 10%) and morbidity.
Acute Suppurative Meningitis Etiology: First 2 months of life: Group B Streptococcus, gram negative bacilli, S. pneumoniae, Neisseria meningitides, Haemophilusinfluenzae type b. and L. monocytogenes. Children 2 mo-12yr of age 1- S. pneumoniae 2- N. meningitides Alterations of host defense: Pseudomonasaeruginosa, Staphylococcus aureus, Salmonella spp., and L. monocytogenes.
*There are 3 main bacterial meningeal pathogens: • Haemophilusinfluenzae • Neisseria meningitides • Streptococcus pneumoniae *Incidence varies by region and age.
Haemophilus influenzae • Small GN, pleomorphic, coccobacilli • H. flu type B causes almost ALL invasive disease • Nontypeable Hib can rarely cause meningitis. • Incidence of Hib decreased by 97% after vaccine
Occurs predominantly in infants 2mo to 2yr of age Many cases are in winter Higher incidence of subdural effusion
Neisseria meningitidis • - GN diplococci • - Serotypes A,B,C,Y, and W135 cause most invasive disease. • - Virulence depends on: • Capsular polysaccharide • LPS(endotoxin) • Pili • IgA protease • ompS gene
Occur in epidemics (type A,C), which is more common in spring, or sporadic all the year (type B,C,Y)
Meningococcus is the only bacterium that frequently causes a rash, which is probably the most important clue to the diagnosis of meningococcal meningitis. It usually begins as a diffuse erythematous maculopapular rash. As the rash evolves, petechiae and purpura appear primarily on the trunk and lower extremities.
Streptococcus pneumoniae • * Small, non-motile GPC in pairs or chains. • * 8 serotypes cause 90% of invasive disease. • 1, 4, 6, 9, 14, 18, 19 & 23 • * Virulence depends on capsular polysaccharides • * Associated with CSF leak (skull fractures), asplenia, HIV, cochlear implants
Young infants ( <1yr) are most susceptible population Peak season: spring and winter Easier to have subdural effusion and hydrocephalus Easily have a protracted course and relapse
Predisposing factors • 免疫功能低下 Immature immunologic function • 血脑屏障不完善(BBB) Immature blood-brain-barrier • 脑脊膜膨出、颅脑手术、颅底骨折等 Impaired blood-brain-barrier
Route of infection Hematogenous dissemination (上感、皮肤感染、腹泻) Adjacent tissue infections (中耳炎、乳突炎、鼻窦炎) brain Congenital malformations (脑脊髓膜膨出、皮毛窦、脑脊液鼻漏)
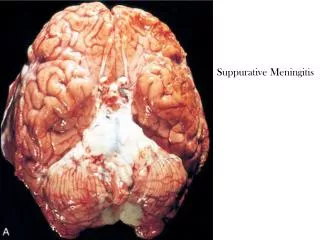
Pathology of suppurative meningitis Purulent exudate of leptomeningitis inflammation( inflammation of pia and arachnoid spaces) over the convexities of the cerebral cortex. This may result in the additional complications of arterial or venous thrombosis with infarction and hemorrhage
The symptoms and signs are not evident in neonates and infants younger than 3mo of age; and patients already received irregular antibiotic therapy.
Nervous system examination Meningeal irritation • Neck stiffness • Kernig sign • Brudzinski sign
Neck stiffness keep the child with supine position without pillow, flex his head, if resistance exists, it means the test is positive.
Kernig sign keep the child with supine position without pillow, flex the hip and knee joint at 90°C, elevate a leg, if the child raises his head or has painful expression, it indicates the test is positive.
Brudzinski sign keep the child with supine position without pillow, flex the head, if the child flexes his legs involuntary at the same time, it means the test is positive.
Diagnosis • Step One: Meningitis, Yes or Not? • Step Two: Meningitis, Which type?
Attention Making Diagnosis As Early As Possible Noticing Atypical Case
Contraindicationsof Lumbar puncture • Severe intracranial hypertension • Circulatory failure • Infection of the puncture site • If there is evident hemorrhage tendency
Diagnosis • Diagnosis is confirmed by analysis of cerebrospinal fluid ( CSF) Suggestion bacterial meningitis • Increased pressure (90%) • Appearance: slightly cloudy to purulent • Raised white blood cells,consisting chiefly of • polymorphonuclear leukocytes • Raised protein concentration, decreased glucose concentration (80%)
Other examination CT/MRI Indication : • Signs of abnormal localization • Treatment is not satisfied • Persistent fever • Head circumference increased • Significantly increased of intracranial pressure EEG Blood Tests, Blood cultures and Chest X-ray
Diagnosis • Earlier diagnosis and prompt initiation of effective antibiotic treatment is critical for minimizing sequelae of purulent meningitis. Suspected cases: febrile infants with seizure, meningeal irritability, increased intracranial pressure, altered mental status Pay attention to the atypical symptoms and signs in neonate, infant and patient alreadyreceived irregular antibiotic therapy
Differential Diagnosis • Viral meningitis or encephalitis • Febrile Seizure • Toxic encephalopathy
MRI scans used in the diagnosisof herpes simplex virus (HSV). MRI typically shows temporal lobe lesions
Treatment Generally, management of viral encephalitis is nonspecific. • Mild case : only symptomatic relief,e.g. fever, headache, vomiting. • Severe case: Require hospitalization and intensive care.
Diagnosis of viral encephalitis • Diagnosis of VE can be confirmed only by finding virus from the brain specimen, but it is carried out only in dead patients. • Diagnosis of VE is relatively confirmed on the clinical presentations ,epidemiologic data, examination of CSF, findings of EEG, and neuroimaging studies.
Febrile Seizure Definition Febrile Seizures are the seizures with fever occurring in children between 6 months to 6 years of age without evidence of intracranial infection or defined cause
Febrile Seizure • Associated with a rapidly rising temperature (usually develop when the temperature reaches 390C or greater ) • Occur with the diseases out side the CNS • Age dependent: 6mon-6year • With normal CNS structure and function • No no-febrile seizure history • Genetic predisposition
Treatment • Routine treatment: • Search for the cause of fever • Control fever (avoid excessive clothing, encourage fluids, tepid sponge bath, and antipyretics)
What to do in emergency Maintain clear airway Roll the child on to one side / prone with head lowered Diazepam 0.3-0.5 mg/kg I.V. Slowly in 2-3 Minutes May be repeated after 5 Minutes Rectal Diazepam (0.5 mg /kg)
Toxic encephalopathy • Seen in severe systemic infection • Can be high fever, delirium, unconsciousness, convulsions and coma • CSF pressure increased while cytological and biochemical tests normal