Download
1 / 29
330 likes | 574 Views
Blood Pressure. Hypertension is a major risk factor for heart disease and stroke. As the first and fourth leading causes of death in the United States. In 2013 about 77.9 million (1 out of every 3) adults have high blood pressure In the US.

E N D
Hypertension is a major risk factor for heart disease and stroke. As the first and fourth leading causes of death in the United States. In 2013 about 77.9 million (1 out of every 3) adults have high blood pressure In the US. Prevalence of hypertension: 28% in the North American countries and 44% in the European countries
A Systematic Review in Iran in 2009: In 30 – 55 years: 23%. More than 55-year-old population: 50% The prevalence in men was 1.3% less than that in women (P<0.0001).
US healthy people 2020 Objectives to reduce the prevalence of hypertension among adults to 26.9% and to increase the prevalence of blood pressure control among adults with hypertension to 61.2% .
Definitions and classification of office BP levels (mmHg)* Hypertension: SBP >140 mmHg ± DBP >90 mmHg
Definition Hypertensive emergency: BP > 180/120 mm Hg and impending or progressive end- organ damage (e.g. neurologic, cardiovascular, eclampsia)
Definition Hypertensive urgency: BP > 180/120 mm Hg without impending or progressive end-organ damage e.g. patient with headache, shortness or breath or epistaxis.
Definition Malignant hypertension: Emergency hypertension + Papilloedema
Epidemiology Incidence of hypertensive emergencies: Declined from 7% to approximately 1% of patients with hypertension. 1-year survival rate : Only 20% prior to 1950, More than 90% with appropriate medical treatment in 2010
Causes The commonest cause of hypertensive emergency in 2011 is undiagnosed, untreated, or undertreated essential Hypertension.
Causes Renovascular, Eclampsia/pre-eclampsia, Acute glomerulonephritis, Pheochromocytoma, Anti-hypertensive withdrawal syndromes, Head injuries and CNS trauma , Drug-induced hypertension, Burns, Vasculitis, Post-op hypertension, Coarctation of aorta
Sign an symptoms The most common clinical presentations: 1- chest pain (27%) 2 - Cerebral infarction (24.5%) 3 – Dyspnea (23%) 4 - Pulmonary edema (22.5%) 5 - hypertensive encephalopathy (16.3%) 6 - congestive heart failure (12%)
CNS - encephalopathy, intracranial hemorrhage, Grade 3-4 retinopathy Heart - CHF, MI, angina • Damage Kidneys - acute kidney injury, microscopic hematuria Vasculature - aortic dissection, eclampsia Vasculature
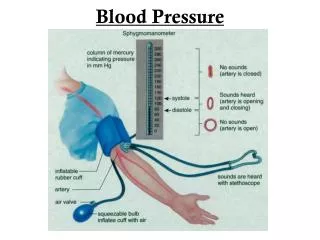
Blood pressure measurement Armstrong study in 2002 in US and Dickson in 2007 in Australia: Findings indicate that knowledge of nurses and nursing students was inadequate to perform blood pressure measurement in a standardized manner.
Blood pressure measurement Studies in Iran also showed similar findings.
Blood pressure measurement Factors affecting the accuracy of blood pressure measurement: 1 – Equipment's error 2 – Patients preparation errors 3 – Examiner errors
Blood pressure measurement Patients preparation errors 1 – Talking or active listening (1 unit increase) 2 – Cuff over clothing ( 0.5 to 5 unit) 3 – Smoking 30 min before (0.6 to 2 unit) 4 – Back unsupported (0.6 to 1 unit) 5 – Arm unsupported (Si) (0.1 to 0.7 unit) 6 – Arm unsupported (St) (0.6 to 0.8 unit)
Blood pressure measurement Patients preparation errors 7 – Pain and anxiety 8 – Distended bladder (increase blood pressure) 9 – Paretic Arm (due to stroke) 10 – patients crosses your legs (0.2 to 0.8 unit increase) 11 – upper arm below or above the atrium level
Blood pressure measurement Examiner errors 1 – Cuff size 2 – Too short rest period ( 5 min) 3 – constrictive clothing around the arm (increased blood pressure) 4 – Caffeine use 5 – Too rapid deflation (decrease blood pressure) 6 – too much cuff inflation (pain and increase blood pressure)
Hypertensive emergency treatment Place patient who is not in distress in a quiet room and reevaluate after an initial interview. In one study, 27% of patients with an initial DBP >130 mm Hg had their DBP fall below critical levels after relaxation without specific treatment.
Hypertensive emergency treatment Screen for end-organ damage: - Patients with end-organ damage usually require admission and rapid lowering of BP using iv meds - Patients without evidence of end-organ effects may be discharged with follow–up
Hypertensive emergency treatment Once the diagnosis of hypertension is made and end organ damage confirmed, the BP should be lowered by about 25% of the mean arterial pressure.
Hypertensive emergency treatment There are 2 main classes of drugs: 1 - Vasodilators 2 - Adrenergic inhibitors
Hypertensive emergency treatment Vasodilators: Nitroprusside (0.25-10mcg/kg/min) Nitroglycerine (5-100mcg/min) Nicardipine (5-15mg/hr) Hydralazine (10-20mg) Enalapril (1.25-5mg1Vq6hr) Fenoldopam (0.1-0.3mcg/kg/min
Hypertensive emergency treatment Adrenergic inhibitors Labetalol (20-80mgiv bolus every 10 min) Esmolol (200-500 mcg/kg/min for 4min) Phentolamine (5-15mg iv)