Download
1 / 59
620 likes | 1.03k Views
SPINAL FUSION AND INSTRUMENTATION. Tae-Hong Lim, Ph.D. Department of Biomedical Engineering The University of Iowa Iowa City, Iowa. Normal Function of the Spine. Protect spinal cord and nerves Support the body weight and external load Stability

E N D
SPINAL FUSION AND INSTRUMENTATION Tae-Hong Lim, Ph.D. Department of Biomedical Engineering The University of Iowa Iowa City, Iowa
Normal Function of the Spine • Protect spinal cord and nerves • Support the body weight and external load • Stability • Allow motion of the body for various activities • Flexibility
Spinal Disorders • Trauma • Fractures, Whiplash injury, etc. • Tumor • Infection & Inflammatory Disease • Deformity • Scoliosis, spondylolisthesis, degenerative lumbar kyphosis, etc. • Cervical & Low-back Pain • Degenerative disease, such as disc herniation, stenosis, spondylolisthesis, etc.
Treatment of Spinal Disorders • Conservative Treatment • Degenerative disease • Stable fracture • Mild deformity • Surgical Treatment • Failed conservative treatment • Unstable fracture (dislocation) • Progressive deformity
Goals of Spine Surgery • Relieve pain by eliminating the source of problems (decompression) • Stabilize the spinal segments after decompression • Restore the structural integrity of the spine (almost normal mechanical function of the spine) • Maintain the correction • Prevent the progression of deformity of the spine
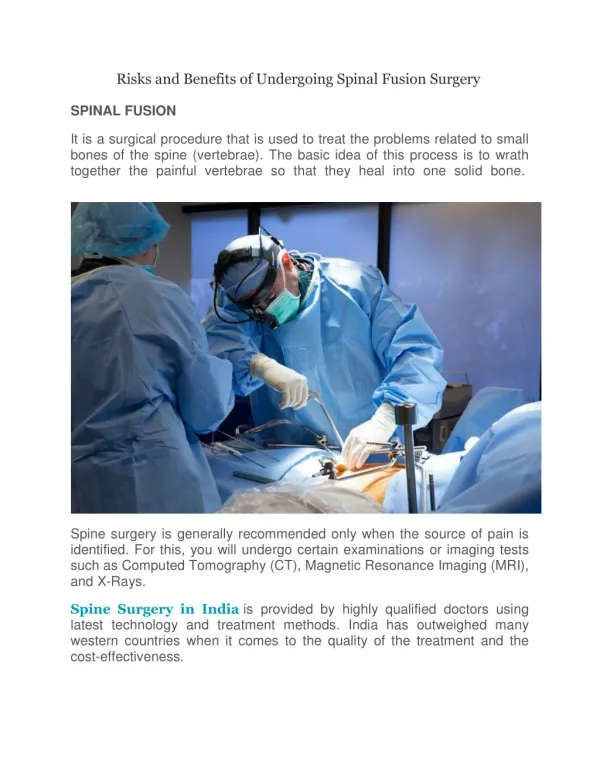
Spinal Fusion • Elimination of segmental movement across an intervertebral segment by bone union • One of the most commonly performed, yet incompletely understood procedures in spine surgery • Non-union rate: 5 to 35 %
Factors for Considerationin Spine Fusion • Biologic Factors • Local Factors: • Soft tissue bed, Graft recipient site preparation, Radiation, Tumor and bone disease, Growth factors, Electrical or ultrasonic stimulation • Systematic Factors: • Osteoporosis, Hormones, Nutrition, Drugs, Smoking • Graft Factors • Material, Mechanical strength, Size, Location • Biomechanical Factors • Stability, Loading
Properties of Graft Materials Graft Osteogenic Oseto- Osteo- Materials Potential induction conduction Autogenous bone o o o Bone marrow cells o ? x Allograft Bone x ? o Xenograft bone x x o DBM x o o BMPs x o x Ceramics x x o DBM = Demineralized bone matrix; BMP = Bone morphogenetic proteins
Spinal Instrumentation • Goals of Spinal Instrumentation: • Correction of deformities or misaligned segments; • Enhancement of solid fusion; • Maintain anatomic alignment until a solid fusion takes place; and • Allow early mobilization of patients by providing an immediate stability
Spinal Instrumentation Types • Implantation Method: • Wiring, Hooks, Screws • Rods vs. Plates • Spinal Level: • Cervical, Thoracolumbar • Position: • Anterior vs. Posterior Instrumentation Vertebra Graft Vertebra Pedicle screw instrumentation
Thoracolumbar Spine Instrumentation Z-plate (Danek) Kaneda (AcroMed)
Operative Techniques • Patient Positioning: • The intra-abdominal pressure must be minimized to avoid venous congestion and excess intraoperative bleeding, while allowing adequate ventilation of the anesthetized patient. • Surgical exposure of the lumbar spine: • Midline incision extended to an additional level
GSFS Implantation Procedure Screw Hole Preparation • Exposure of the junction between the pars interarticularis and transeverse processes • Pedicle entrance point is at the crossing of two lines • Vertical line: 2-3 mm lateral from the pars and slants slightly from L4 to S1. • Horizontal line passes through the middle of the insertion of the transverse processes or 1-2 mm below the joint line. • 1-2 mm lateral from the center of the pedicle to insert the screw without disturbing the facet joint above and to medialize the screw for better fixation.
GSFS Implantation Procedure Screw Hole Preparation Angle and depth of the screw holes?
GSFS Implantation Procedure Preparation of Fusion Bed and Grafting • Decortication • Marking screw holes • Grafting
GSFS Implantation Procedure Screw Selection and Insertion • Screw Diameter: • approx. 80% of the medial diameter of the pedicle • Perforation of the pedicle into the medial or inferior side has higher chance of nerve root injury. • Screw Length: • Long enough to pass the half of the vertebral body but • Short enough not to penetrate the anterior cortex Screw Length For GSFS
GSFS Implantation Procedure Rod-Connector-Screw Assembly • Rod Length: - Rod length must not be too long so that the proximal tip of the rod do not touch the inferior facet of the upper vertebra. • Rod Bending • Connector Selection • Rod-Connector Assembly • Screw-Connector-Rod Assembly • Tightening the nuts and set screws
Rod-Screw Assembly • Medial-lateral adjustability can eliminate: • The use of additional components; and • Application of force in medial-lateral directions or additional rod bending • In order to make the rod-screw connection
GSFS Implantation Procedure Rod-Connector-Screw Assembly GSFS: - Screw-Connector: Polyaxial - Connector Length:M-L Adjustment *No precise rod-bending is required. *Screw alignment is not as critical.
GSFS Implantation Procedure Rod-Connector-Screw Assembly • Rod-bending; • Insert the rod to the connectors; • Temporary tightening of set screws of the proximal and distal most connectors; • Place the rod-connector assembly on the screws; • Tightening the screw caps and set-screws in the proximal and distal most connectors while holding the rod in a desired shape; and • Fix the other screw caps and set-screws in the mid-portion.
Ideal Features • The use of connectors: • Polyaxial and medial-lateral adjustability; • No need for precise rod bending • Easy screw-rod connection without a good alignment of screw heads • Screw insertion according to the best possible anatomic conditions • Rigid connection at rod-connector and screw-cap connection: • Strong maintenance of correction • Better mechanical environment to enhance bone healing (fusion) • Top-tightening: • Low Assembly profile:
Consideration Factors in Spinal Instrumentation • Materials: • Bio-compatibility and Imaging compatibility • Stiffness (or elasticity) and strength • Corrosion • Implant Strength: • Component (screw, rod, plate, wire, etc.) strength • Metal-metal interface strength • Construct strength • Bone-metal interface strength: Bone–wire, -hook, and -screws • Construct Stability: • Segmental stiffness or flexibility • Profile: • Ease of Use:
Spinal Implant Materials • 316L Stainless steel: • Biocompatible • Strong and stiff • Poor imaging compatibility: artifact to CT and MRI • Titanium Alloy (Ti6Al4V ELI): • Biocompatible • No artifacts during CT and MRI • Excellent fatigue strength, high strength, high elasticity • High resistance to fretting corrosion and wear (surface treatments)
Spinal Implant Strength • Static and Fatigue Strength of Components: • Depends on the material properties, size and shape of the components • Metal-metal Interface Strength: • Rod-screw connections • GSFS (rod-connector and screw-connector interfaces): excellent • Construct Strength: • Excellent in GSFS
Bone-Metal Interface Strength • Pedicle screws are known to provide the strongest bone purchase compared to wires, hooks, and vertebral screws. • Screw Pullout Strength: • Affected by major diameter and bone quality (BMD) but not by minor diameter, thread type, and thread size. • Insertion depth is not critical. • Screw insertion torque was known to have relationship with screw pullout strength. • Conical screws showed similar pullout strength to that of the cylindrical screws.
Surgical Construct Stability • Construct stability varies depending on the size of the screws and rods (plates). • Recommended rod diameter is 6 mm or ¼ inch in adult spine surgery. • Preservation of more than 70% of the disc or meticulous anterior grafting is critical to obtain stable construct with no hardware failure (screw or rod breakage). • Modern spinal fixation systems, regardless of anterior or posterior fixation, similarly significant stability in flexion, extension, and lateral bending, but not effective in preventing axial rotational (AR) motion. • Use of a crosslink (DDT) is recommended to improve the AR stability, particularly in the fixation of long segments (more than 2 levels).
Surgical Construct Stability EXT • Ligamentous spines • Pure moment • in FLX, EXT, LB, and AR • Maximum 8.2 Nm • 3-D motion analysis system AR LB FLX L2 FLX LB AR EXT L5
Implant Assembly Profile • Anterior Instrumentation: • Critical in anterior plating of the cervical spine, and the profile must be less than 3 mm. • Lower profile is recommended in the anterior fixation of the thoracolumbar spine. • Posterior Instrumentation: • Assembly profile is not as critical as in anterior fixation, but lower profile is recommended because a high profile may cause a surgery for implant removal due to patients’ uncomfortness.
Ease of System Assembly • Screw Insertion: • Screw insertion according to the best possible anatomic orientation and location • Adjustment in Screw-Rod Assembly: • Rod bending • Angular adjustment • Medial-lateral adjustment • Polyaxial screw head vs. Connector • Top-tightening • All assembly procedures can be made from the top.
BIOMECHANICAL EVALUATION OF DIAGONAL TRANSFIXATION IN PEDICLE SCREW INSTRUMENTATION Tae-Hong Lim, Ph.D. Atsushi Fujiwara, M.D. Jesse Kim, B.S. Timothy T. Yoon Sung-Chul Lee, M.D. Howard S. An, M.D.
Horizontal Transfixation (HTF) • Construct stability • No improvement in FLX and EXT • Some improvement in LB • Significant improvement in AR • Increased AR stability when using 2 transfixators • Optimum position for TF • Proximal 1/4 points for 1 TF • Proximal 1/8 and middle points for 2 TF Lim et al. 1995 Transfixator (TF) VB VB Pedicle screw instrumentation
Diagonal Transfixation (DTF) • Construct stability • No changes in FLX (Texada et al, 1999) • Significant improvement in LB and AR (Texada et al., 1999; McLain et al. 1999) Transfixator (TF) VB VB Pedicle screw instrumentation
Diagonal Transfixation (DTF) • Clinical application of DTF using 2 TFs may not be practical. • Limited space • Higher construct profile • DTF using 1 TF is feasible, but its effect has not been investigated yet.
PURPOSE • To evaluate the effect of diagonal transfixation (DTF) on the construct stability and the corresponding stress changes in the pedicle screw in comparison with the effect of horizontal transfixation (HTF)
Flexibility tests • Unstable Calf Spine Model • Finite element studies
FLEXIBILITY TESTS EXT • 10 Ligamentous calf spines (L2-L5) • Pure moment • in FLX, EXT, LB, and AR • Maximum 8.2 Nm • 3-D motion analysis system AR LB FLX L2 FLX LB AR EXT L5
Tested Constructs - Intact - Instrumentation without TF after total discectomy (no TF) - Instrumentation with HTF using 1 TF (HTF) - Instrumentation with DTF using 1 TF (DTF) Diapason Spinale Fixation System (Stryker, Allendale, NJ: 6.5 mm screws and 6 mm rods and TF)
Finite Element Studies • To investigate the stress changes in the pedicle screws due to HTF and DTF. • Boundary and Loading Conditions: • Nodes in lower vertebra were held fixed. • FLX, EXT, LB, and AR Moments (8.2 Nm) at the middle point of the vertebra element • ADINA Finite Element Analysis S/W
Fixed Nodes Finite Element Models Moment Moment Vertebrae Transfixators (A) Horizontal transfixation (HTF) (B) Diagonal transfixation (DTF)
Data Analysis • Rotational motion of L3 with respect to L4 in response to 8.2 Nm • Rate of motion change with respect to • Intact case • No TF case • Total load = [Mx2 + My2 + Mz2]1/2 • Mx = Torsional moment; My & Mz = Bending moments • Stress change changes in total load