Download
1 / 1
10 likes | 142 Views
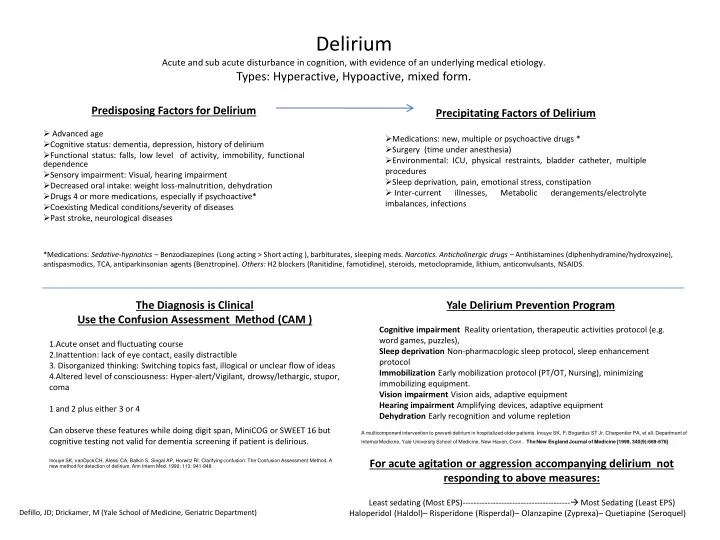
Precipitating Factors of Delirium Medications: new, multiple or psychoactive drugs * Surgery (time under anesthesia) Environmental: ICU, physical restraints, bladder catheter, multiple procedures Sleep deprivation, pain, emotional stress, constipation

E N D
Precipitating Factors of Delirium • Medications: new, multiple or psychoactive drugs * • Surgery (time under anesthesia) • Environmental: ICU, physical restraints, bladder catheter, multiple procedures • Sleep deprivation, pain, emotional stress, constipation • Inter-current illnesses, Metabolic derangements/electrolyte imbalances, infections DeliriumAcute and sub acute disturbance in cognition, with evidence of an underlying medical etiology.Types: Hyperactive, Hypoactive, mixed form. *Medications: Sedative-hypnotics – Benzodiazepines (Long acting > Short acting ), barbiturates, sleeping meds. Narcotics. Anticholinergic drugs – Antihistamines (diphenhydramine/hydroxyzine), antispasmodics, TCA, antiparkinsonian agents (Benztropine). Others: H2 blockers (Ranitidine, famotidine), steroids, metoclopramide, lithium, anticonvulsants, NSAIDS. The Diagnosis is Clinical Use the Confusion Assessment Method (CAM ) Acute onset and fluctuating course Inattention: lack of eye contact, easily distractible Disorganized thinking: Switching topics fast, illogical or unclear flow of ideas Altered level of consciousness: Hyper-alert/Vigilant, drowsy/lethargic, stupor, coma 1 and 2 plus either 3 or 4 Can observe these features while doing digit span, MiniCOG or SWEET 16 but cognitive testing not valid for dementia screening if patient is delirious. Inouye SK, vanDyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: The Confusion Assessment Method. A new method for detection of delirium. Ann Intern Med. 1990; 113: 941-948. Yale Delirium Prevention Program Cognitive impairment Reality orientation, therapeutic activities protocol (e.g. word games, puzzles), Sleep deprivation Non-pharmacologic sleep protocol, sleep enhancement protocol Immobilization Early mobilization protocol (PT/OT, Nursing), minimizing immobilizing equipment. Vision impairment Vision aids, adaptive equipment Hearing impairment Amplifying devices, adaptive equipment Dehydration Early recognition and volume repletion Predisposing Factors for Delirium Advanced age Cognitive status: dementia, depression, history of delirium Functional status: falls, low level of activity, immobility, functional dependence Sensory impairment: Visual, hearing impairment Decreased oral intake: weight loss-malnutrition, dehydration Drugs 4 or more medications, especially if psychoactive* Coexisting Medical conditions/severity of diseases Past stroke, neurological diseases A multicomponent intervention to prevent delirium in hospitalized older patients. Inouye SK, F; Bogardus ST Jr, Charpentier PA, et all. Department of Internal Medicine, Yale University School of Medicine, New Haven, Conn .The New England Journal of Medicine [1999, 340(9):669-676] For acute agitation or aggression accompanying delirium not responding to above measures: Least sedating (Most EPS)--------------------------------------- Most Sedating (Least EPS) Haloperidol (Haldol)– Risperidone (Risperdal)– Olanzapine (Zyprexa)– Quetiapine (Seroquel) Defillo, JD; Drickamer, M (Yale School of Medicine, Geriatric Department)