Download
1 / 26
260 likes | 395 Views
Alabama SHRM Tusculoosa , AL 10/20/11 Brian Klepper. What If Employers Walked Away From Health Coverage?. Cumulative Increases in Health Insurance Premiums, Workers’ Contributions to Premiums, Inflation, and Workers’ Earnings, 1999-2011.

E N D
Alabama SHRM Tusculoosa, AL 10/20/11 Brian Klepper What If Employers Walked Away From Health Coverage?
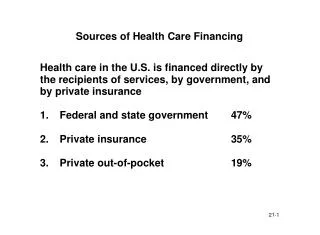
Cumulative Increases in Health Insurance Premiums, Workers’ Contributions to Premiums, Inflation, and Workers’ Earnings, 1999-2011 Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 1999-2011. Bureau of Labor Statistics, Consumer Price Index, U.S. City Average of Annual Inflation (April to April), 1999-2011; Bureau of Labor Statistics, Seasonally Adjusted Data from the Current Employment Statistics Survey, 1999-2011 (April to April).
Percentage of All Firms Offering Health Benefits, 1999-2011 *Estimate is statistically different from estimate for the previous year shown (p<.05). Note: Estimates presented in this exhibit are based on the sample of both firms that completed the entire survey and those that answered just one question about whether they offer health benefits. The percentage of firms offering health benefits is largely driven by small firms. The large increase in 2010 was primarily driven by a 12 percentage point increase in offering among firms with 3 to 9 workers. In 2011, 48% of firms with 3 to 9 employees offer health benefits, a level more consistent with levels from recent years other than 2010. The overall 2011 offer rate is consistent with the long term trend, indicating that the high 2010 offer rate may be an aberration. Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 1999-2011.
Average Annual Health Insurance Premiums and Worker Contributions for Family Coverage, 2009-2011 $15,073 $13,770 $13,375 Worker Contribution Employer Contribution Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits, 2009-2011.
Health Care’s Growing Burden on Federal Budget Crowds Out Other Needs, Like Education
Here’s the Projected Percentage of the Larger Economy
Will Employers Drop Health Coverage • In Favor of Health Care Exchanges? • McKinsey & Co (6/11) – All Employer Sizes • 30%will definitely or probably drop it. • >50% -60% of employers withhigh reform awareness will drop it or pursue major change. • Mercer (6/11) – Large and Small Employers • 8% Will Drop It • Avalere Health (6/11 Survey: Urban Institute, RAND Corp, CBO, Lewin) • -0.3% - 8.4% Change from Baseline without PPACA • Towers-Watson (7/11) - Mid-Sized and Large Employer • 10% Will Drop It. • Another 1 in 5 Is Unsure
Best Guess (But Nobody Really Knows) • Most Mid-Sized and Large Employers Will Wait and See • Probably Many More Smaller Firms Will Drop Coverage
Two Scenarios Against a Bleak Economic Backdrop Republicans Win Health Industry Backs Republicans in Opposing HC Reform Health Law’s Cost Control Provisions Neutralized Egregious Practices (e.g., Unnecessary & Inappropriate Utilization) Intensify Employers Rapidly Priced Out of HC Market Health Care/Coverage Sectors Implode Pressure Increases on Gov’t For Solution.
Two Scenarios Against a Bleak Economic Backdrop Democrats Win Health Care Reform Law Moves Forward 2014 Health Care Exchanges Become Active Economy Still Sluggish, HC Costs Still Increasing Smaller Businesses, Particularly, See the Business Sense in Moving Employee Coverage to Exchanges
Some Business Decision Arithmetic • Let’s Say: • Avg Employer HC Cost/EE is $10K • For $6K (including $2,000 + Other Fees), Employees Moved to Exchange • Strong Incentive = Mass Migration • For Argument’s Sake, Say 50% of Workers Move To Exchanges
Some Business Decision Arithmetic In the US Health System in 2010: We Spent About $2.6 Trillion About Half ($1.3 Trillion) Was For Commercial Coverage Employers Paid $1 Trillion Workers Paid $300 Billion In Exchange Example, Employer Cost (Subsidy) Drops $200 Billion Annually, to $800 Billion.
What Happens To the $200 Billion/Year? • Does the Industry Simply Shrink? Not Willingly • Does Government Cover It? With What? • $200 Billion Annually in New Taxes To Cover The Subsidy Would Equal to 2.5x the 2009 Wall St. Bailout/Economic Stimulus Package. Not Likely. • Are We Stuck?
Market-Based Reforms • Over the past 20 years, employers (& health plans) have: • Significantly increased copaysfor “steerage.” • Introduced generic drugs and mail-order. • Introduced Wellness, DM, Lifestyle Coaching • Introduced Incentives • Renegotiated network discounts. • Given employees “more skin in the game.”
Market-Based Reforms Over the past 20 years, we mostly haven’t: Managed the care process, like businesses would.
Major Health Care Structural Flaws • Fee-For-Service Reimbursement • Lack of Pricing/Quality/Safety Transparency • Subjugation of Primary Care
Unaligned Incentives When an employer sits down at the table with his health care relationships – the broker, health plan, doctor, hospital, drug and device company – everyone in the room but him wants it to cost more, and they’re positioned to make that happen. Lynn Jennings, CEO WeCare TLC, LLC
Unnecessary/Inappropriate Care & Cost Our research found that wasteful spending in the health system has been calculated at up to $1.2 trillion of the $2.2 trillion (54.5%) spent in the United States. [R]edundant, inappropriate or unnecessary tests and procedures [were] identified as the biggest area of excess, followed by inefficient healthcare administration and the cost of care necessitated by conditions such as obesity, which can be considered preventable by lifestyle changes. The Price of Excess PricewaterhouseCoopers, 2008
Market-Based Approaches That Work • Empowering Primary Care • Data Collaboratives • Medical Destinations • New Technologies (e.g., Minimally Invasive Procedures, Genomics) • Patient Engagement • Rx Step Therapies • Lifestyle Management/Obesity Step Therapies • Employer Leadership
What Happened in Lafayette, IN • Relatively small community with high concentration of mid-sized/large employers (e.g., Subaru factory, Purdue University). • 2nd highest health care costs in IN • Employers came together 6 years ago, pursued clinics, changed the market. • This can work anywhere.
The Employer’s Dilemma “We decided to stop letting the providers take advantage of us.” Jane Wolfe Benefits Manager Fairfield Manufacturing Lafayette, IN
Effective Onsite/Nearsite Clinic Characteristics • Outside FFS, So No Financial Conflicts • Advanced Primary Care Medical Homes • Comprehensive Medical Management Platforms That Incorporate Other Key Mgmt Approaches and Influence Care Throughout The Continuum. • Group Health Savings of 25%-35% Year 1, Net of Clinic Cost, While Reducing Population-Level Health Risk
Onsite/Nearsite Clinics – Competitive Advantage Savings Grow Over Time, and Create Competitive Advantage Illustrative Only
Brian R. Klepper, PhD is a health care analyst, industry advisor and commentator. He is Chief Development Officer for WeCare TLC, LLC, an onsite primary care clinic and medical management firm based in Longwood, FL and Managing Principal of Healthcare Performance Inc., a consulting practice based in Atlantic Beach, FL. An active author and speaker, Dr. Klepper has provided health care commentary to CBS Evening News, the Wall Street Journal, the New York Times, and the Washington Post. He has published articles on Kaiser Health News, Medscape, Healthleaders, The New England Journal of Medicine, Modern Healthcare, Business Insurance and newspapers nationally. In December 2010, he founded and now edits Care & Cost, an online professional health care magazine and forum. In February 2011, he founded Replace the RUC!, an effort focused on the most important driver of inappropriate health care cost. He is a regular columnist on the Health Affairs Blog,and other expert health care blogs. Brian is a Committee Chair on the recently convened American Academy of Family Physicians’ Primary Care Services Valuation Task Force, and a reviewer for Health Affairs and The Journal of Ambulatory Care Management. He serves on the Boards of the Lundberg Institute and the Consortium for Southeast Hypertension Control (COSEHC), dedicated to translational medicine for vascular disease. He is an Advisor tothe Patient-Centered Primary Care Collaborative, which advocates for medical homes, and the Center for Value Health Innovation, which helps business identify and implement approaches that have been proven to improve quality and safety while reducing cost. Contact Brian at 904.343.2921, bklepper@gmail.com.