Download
1 / 32
330 likes | 590 Views
Integration of EGFR targeting into first line therapy: is it time?. Prof Eric Van Cutsem, MD, PhD Leuven, Belgium. The Epidermal Growth Factor Receptor pathway. Scaltriti M & Baselga J. Clin Cancer Research 2006. Anti-EGFR antibodies in mCRC. cetuximab + irinotecan (n=218).

E N D
Integration of EGFR targeting into first line therapy: is it time? Prof Eric Van Cutsem, MD, PhD Leuven, Belgium
The Epidermal Growth Factor Receptor pathway Scaltriti M & Baselga J. Clin Cancer Research 2006
cetuximab + irinotecan (n=218) cetuximab (n=111) Cetuximab +/- irinotecan in irinotecan refractory EGFR+ mCRC: Response rate (primary endpoint) 56[49-62] ** 60 50 * 32[24-42] 40 Percentage 23[18-29] 30 11[6-18] 20 10 0 Response Rate Disease Control(CR+PR+SD) * p=0.0074; ** p<0.001; [] = 95% CI Cunningham D … Van Cutsem E. N Engl J Med 2004
Cetuximab and panitumumab in chemorefractory EGFR expressing CRC ¹Van Cutsem E et al, J Clin Onc 2007; ²Jonker D et al, N Engl J Med 2007; ³ Amado R, Van Cutsem E et al; Eur J Cancer (Proc ECCO), 2007
EPIC trial: Cetuximab in second line treament of mCRC Sobrero A et al. AACR 2007
Anti-EGFR antibodies in first line treatment of mCRC • Phase II studies: high response rates and high disease control rates • Fluoropyrimidine/irinotecan + cetuximab • Fluoropyrimidine/oxaliplatin + cetuximab • Randomized phase II studies • CALGB • Opus • SAKK • BOS - EORTC • Randomized phase III studies • COIN: 3 arm question on duration and on ± cetuximab • CAIRO-2: XELOX/bevacizumab ± cetuximab • US intergroup: 3 arm: bevacizumab vs cetuximab vs combination • Nordic: FOLFOX ± cetuximab • FOLFOX ± panitumumab • …….
Advanced Colorectal Cancer:CALGB 80203 + cetuximab RANDOMI ZAT ION n = 238/2200 FOLFIRI - cetuximab Stratify Prior adj Prior XRT + cetuximab FOLFOX - cetuximab Venook A et al ASCO 2006
CALGB 80203: Response Cetuximab - / + p = 0.029; chi-sq p = 0.029; chi-sq Venook A et al ASCO 2006
SAKK Phase II Study: Preliminary Results Helbling D, et al. ESMO 2006 A328 AIO CRC Study Group Phase II First-Line study Heinemann V, et al. ASCO GI, 2007
OPUS trial in first line mCRC: large randomized phase II study Bokemeyer C, et al. ECCO 2007 (Abstract No. 3004)
OPUS: safety aIncludes peripheral sensory neuropathy and neuropathy bThere were no grade 4 skin reactions or acne-like rash Magnesium measurements were available only from a subset of patients Bokemeyer C, et al. ECCO 2007 (Abstract No. 3004)
COIN trial: Phase III study Previously untreated patients with mCRC • UK National Cancer Research Institute study, 84 participating centers • Current accrual: 1800 (n=2421 planned) • Preliminary safety analysis on 804 patients randomized up to June 20061 Cetuximab + oxaliplatin/5-FU or capecitabine Oxaliplatin + 5-FU or capecitabine R Intermittent oxaliplatin + 5-FU or capecitabinea a12 weeks, monitor and repeat on PD 1Maughan T, et al. ASCO 2007 (Abstract No. 4070)
COIN trial: Any Grade 3 /4 toxicity (%) in the first 12 weeks † † † = p<0.001 compared to same regimen minus cetuximab 1Maughan T, et al. ASCO 2007 (Abstract No. 4070)
COIN study: Chemo-type toxicities (%) in the first 12 weeks No cetuximab (Arms A + C) Cetuximab (C) (Arm B) Significance * p<0.05 † p<0.001 Regimen Ox + Cap OxMdG Ox + Cap OxMdG +/- cap +/- cet n 333 203 166 102 Neutropenia 2 18 1 26 † N & vomiting 7 3 14 7 * * Diarrhoea 15 7 25 13 † * All cause 60 day mortality 5.65 5.0 7.2 4.9 Treatment related deaths 0.6 0.5 1.8 1.0 1Maughan T, et al. ASCO 2007 (Abstract No. 4070)
CRYSTAL trial in first line mCRC Cetuximab + FOLFIRI Cetuximab IV 400 mg/m2 on day 1, then 250 mg/m2 weekly+ irinotecan (180mg/m2) + 5-FU (400 mg/m2 bolus + 2400 mg/m2 as 46-hr continuous infusion) + FA every 2 weeks Stratification factors: • Regions • ECOG PS Populations • Randomized patients n=1217 • Safety population n=1202 • ITT population: n=1198 EGFR-expressing metastatic CRC R FOLFIRI irinotecan (180 mg/m2) + 5-FU 400 mg/m2 bolus + 2400 mg/m2 as 46-hr continuous infusion) + FA every 2 weeks Van Cutsem E, et al. Proc ASCO, 2007
0.9 Cetuximab + FOLFIRI, n=599 0.8 FOLFIRI, n=599 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0 0 2 4 6 8 10 12 14 16 18 20 Subjects at risk FOLFIRI alone 599 492 402 293 178 83 35 16 7 4 1 Cetuximab + FOLFIRI 599 499 392 298 196 103 58 29 12 5 1 CRYSTAL trial: Primary endpoint PFS ITT population independent review 1.0 HR = 0.851; 95% CI = [0.726-0.998] Stratified log-rank p-value = 0.0479 8.9 mo PFS estimate 1-year PFS rate 23% vs 34% 8.0 mo Progression-free survival time (months) Van Cutsem E, et al. Proc ASCO, 2007
FOLFIRI alone Cetuximab + FOLFIRI 10 9.8 9 8 7 6 Percentage (%) 5 4 4.5 3 2 1 0 No residual tumor in patients with liver metastases n=134/n=122 CRYSTAL trial: Response Rate and Surgery with curative intent Liver metastases only population(exploratory) ITT population(pre-planned) p=0.0034* odds ratio 3.0 [95% CI: 1.4 - 6.5] *CMH test Van Cutsem E, et al. Proc ASCO, 2007
CRYSTAL trial:Safety: Grade 3/4 AE aThere were no grade 4 skin reactions Magnesium levels were measured in only 20% of the patients (0.2% vs. 1.8%) Van Cutsem E, et al. Proc ASCO, 2007
PACCE: Panitumumab Advanced Colorectal Cancer Evaluation Randomized, Open-Label, Controlled Phase 3b Trial Panitumumab 6 mg/kg Q2W Ox-CT Bevacizumab Ox-based CT (eg, FOLFOX) N = 800 Inv choice S C R E E N I N G R A N D O M I Z E 1:1 Ox-CT Bevacizumab Panitumumab 6 mg/kg Q2W Iri-CT Bevacizumab Iri-basedCT (eg, FOLFIRI) N = 200 Inv choice 1:1 Iri-CT Bevacizumab Stratification Factors: ECOG score, prior adjuvant tx, disease site,Ox doses/Iri regimen, number of metastatic organs Hecht R et al, Ann Oncol, WCGIC Barcelona 2007
pmab+bev/Ox-CT bev/Ox-CT PACCE trial: Progression-free Survival: Ox-CT Cohort(Interim Analysis, May 2007 Data Cutoff) Local Reviewb Central Reviewa HR = 1.27 (95% CI: 1.07–1.50)* HR = 1.27 (95% CI: 1.05–1.53)* *Descriptive only *Descriptive only bCensoring based on last day of patient contact or visit Q2W aCensoring based on last available scan read centrally Q12W Hecht R, Mitchel E et al, GI Cancers Symposium, Orlando, jan 2008
CALGB 80405 trial: Phase III study FOLFOX or FOLFIRI, and bevacizumab Previously untreated patients with mCRC FOLFOX or FOLFIRI, and cetuximab R FOLFOX or FOLFIRI, bevacizumab and cetuximab • Primary endpoint: overall survival • Secondary endpoints include response, PFS, toxicity and resection rate • Accrual = 1084/2289 • No safety concerns (regular IDMC review)
CAIRO-II trial: Phase III study Cetuximab + bevacizumab + XELOX Previously untreated patients with mCRC • Accrual complete (n=755) • Interim safety analysis (n=381) reported acceptable AEs in both treatment groups • Except for cetuximab-associated skin reactions, there was no difference in the incidence of grade 3/4 AEs between treatment groups R Bevacizumab + XELOX Tol J, et al. ECCO 2007 (Abstract No. 3000)
CAIRO-2 studyOverall toxicity Tol J, et al. ECCO 2007 (Abstract No. 3000)
Resect ion EORTC phase II BOS study Previously untreated patients with resectable mCRC (liver) Adjuvant therapy for 3 months(same schedule as pre-operatively) FOLFOX + cetuximab for 3 months (n=50) R FOLFOX + cetuximab + bevacizumab for 3 months (n=50) Neoadjuvant therapy
EGFR inhibitors in mCRC: questions & challenges • Optimal cytotoxic partner? • Optimal setting: more advanced disease or first line treatment? • Predictive markers for response and activity? • Selection of patients? • Prediction of and decreasing toxicity? • Relevance of correlation skin toxicity and efficacy • What is the clinical significance of increased resection rate of metastases with cetuximab in first line ? • Can EGFR antibodies be combined with other biologics? • bevacizumab? • How can we explain negative results of chemo + bevacizumab and panitumumab in first line? • Economic burden
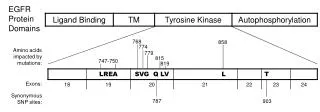
Patient Selection After EGFR Inhibitors • Skin rash • EGFR - IHC • Downstream markers? • Gene Mutations • KRAS • EGFR gene copy number, as assessed by FISH ? • Ligands: amphiregulin, epiregulin • …
Cetuximab / panitumumab and K-RAS Khambata-Ford S et al, J Clin Onc 2007
Mutant Wild-Type 160 160 140 140 PR (0%) SD (12%) PD (70%) PR (17%) SD (34%) PD (36%) 120 120 100 100 80 80 60 60 Pmab + BSC % Change % Change 40 40 20 20 0 0 -20 -20 -40 -40 -60 -60 -80 -80 Patient Patient 160 160 140 140 PR (0%) SD (8%) PD (60%) PR (0%) SD (12%) PD (75%) 120 120 100 100 80 80 60 60 BSC Alone 40 40 % Change % Change 20 20 0 0 -20 -20 -40 -40 -60 -60 -80 -80 Patient Patient Chemorefractory patients: Panitumumab + BSC vs BSCMaximum Percent Decrease in Target Lesions Final Analysis, KRAS Evaluable Group Amado R, Van Cutsem E et al, J Clin Oncol 2008, in press
First line treatment with cetuximab First line treatment: cetuximab (n = 33) Response rate: 10 %; Stabile disease: 34% Pessino A, Sobrero A et al, Ann Oncol epub 2007 First line treatment: cetuximab followed by FOLFIRI/cetuximab (n = 52) Tabernero J et al, GI Cancers symp 2008
Anti-EGFR antibodies in first line treatment of mCRC • Specific issues/questions? • Do anti-EGFR antibodies increase the activity of chemotherapy in first line? yes (cetuximab trial), but which subgroup? no data in comparison with bevacizumab • Do anti-EGFR antibodies increase the toxicity? yes Is the toxicity in first line acceptable? Is there an interaction between panitumumab and bevacizumab? • Is KRAS a predictive marker for activity in first line in combination with chemotherapy? more data expected • Does cetuximab increase the resection rate in first line metastatic CRC? probably yes
EGFR inhibitors in CRC • Are EGFR inhibitors an option in first line treatment of mCRC? • Probably yes • For who? • Biomarker or clinically driven selection? • Data: • Cetuximab • Panitumumab under evalution • Are EGFR inhibitors today a standard treatment in first line mCRC? • No