Download
1 / 33
350 likes | 1.2k Views
Minimizing Opioids in the Perioperative Period. Trina M. Kleiver MD Assistant Professor Director of Acute Pain & Regional Anesthesia Department of Anesthesiology University of Arkansas for Medical Sciences. Disclosures. No financial disclosures. Objectives.

E N D
Minimizing Opioids in the Perioperative Period Trina M. Kleiver MD Assistant Professor Director of Acute Pain & Regional Anesthesia Department of Anesthesiology University of Arkansas for Medical Sciences
Disclosures • No financial disclosures
Objectives • Defining the opioid epidemic as it relates to perioperative opioid use • Discuss Enhanced Recovery After Surgery (ERAS) and what it encompasses • Discuss Multimodal Analgesia perioperatively • Discuss Regional Anesthesia and how it can be utilized to decrease opioid use perioperatively • Review components of ERAS and discuss how it all fits together
Why are opioids bad? Sedation Hypotension Respiratory depression Death • Hyperalgesia • Increased sensitivity to pain • Mins to hrs of exposure to opioids leads to this for 24 hours or more • Addiction • Immunosuppression • Ileus • Constipation • Nausea/vomiting • Hormonal Levels
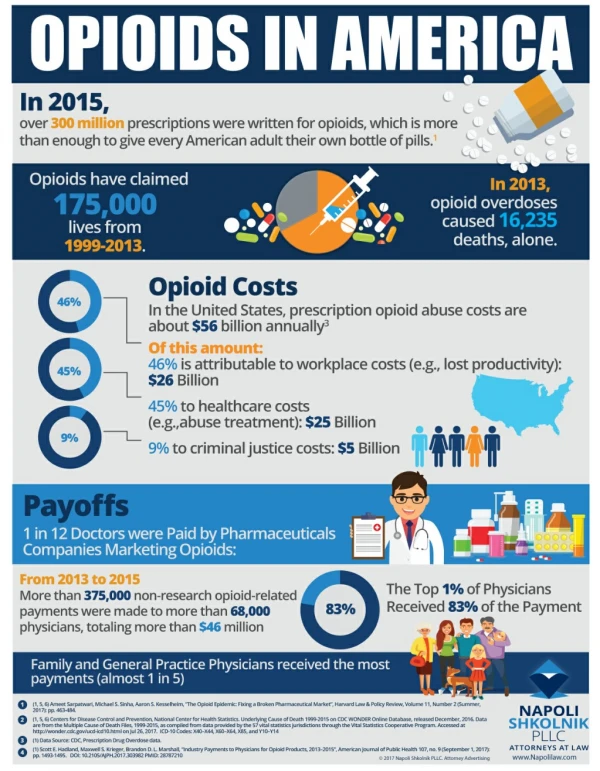
The Opioid Epidemic • Millet et al, 2016 described association between initial opioid prescribing patterns and subsequent long term use in opioid-naïve patients • Looked at 536K patients • Of those 26K (5%) patients become long term users (LTU) • LTU’s were 7x more likely to be hospitalized • Increased number script fills increase likelihood to become LTU • Single script for long acting opioid increased likelihood to become LTU by 16% • Risk Factors • Increasing age • Rural areas
Opioid epidemic continued • How do we stop more people from becoming LTUs? • More selective opioid use—short acting agents • Lower doses • Fewer days supply, No refills • Cumulative dose < 120 Morphine mg equivalents • CDC recommends 3-7 day supply • What happens to the left over opioids? • 80% of people start their opioid use with unused opioids from family or friends • How do we reduce the risk of patients becoming LTUs for acute pain from trauma or surgery?
Enhanced Recovery After Surgery(ERAS) • Perioperative Pathway • Preoperative--days prior to surgery up to patient arrival in OR • Intraoperative • Postoperative—recovery room to discharge from hospital and beyond • Developed by anesthesiologists and surgeons • Evidence based interventions
Introduction to ERAS Multidisciplinary Multifocal Preoperative medication Preoperative nutrition & conditioning Preoperative NPO status/volume status Intraoperative anesthesia management Postoperative pain control Other postoperative management • Primary care physician • Surgeon • Anesthesiologist • Acute pain service • Physical & occupational therapy • Nutritionist • Pharmacist • Nursing staff
Anesthesia Components of ERAS Preoperative Intraoperative Postoperative Preoperative phone call & visit NPO status Normothermia Multimodal analgesia Opioids +/- Thoracic epidural +/- preoperative block or peripheral nerve catheter Normothermia Euvolemia Medications Ketamine Lidocaine +/- Iv acetaminophen Toradol Dexamethasone Dexmedetomidine Esmolol Type of anesthesia Blocks or catheters post-induction or in OR prior to emergence Normothermia Postoperative blocks or catheters Consider same medications as preopplus Diazepam (Valium) Ketamine infusion Lidocaine patch
Preoperative Components of ERAS • Preoperative phone call & visit, nutrition, conditioning • NPO status • Minimize NPO status, • Generally: 2 hours clear liquids, 8 hours solids • Normothermia • Pre-warm in preoperative area • Hypothermia contributes to: • Surgical site infections • Myocardial ischemia • Increased intraoperative blood loss/bleeding diatheses • Prolonged drug effects • Shivering • Skin integrity, pressure ulcer formation
Preoperative Components of ERAS (continued) • Multimodal analgesia • Acetaminophen • usually given po, much less expensive than iv • Contraindications: cirrhosis • Gabapentin • NMDA receptor antagonist • Dose for CrCl > 60 = 900mg • Dose for CrCl <60 or age >65 = 600mg • NSAID • ibuprofen, meloxicam (Mobic), celecoxib (Celebrex) • Contraindications: CrCl < 30, Gi bleed, PUD, h/o CABG • +/- Scopolamine patch • Contraindications: Age > 65, narrow angle glaucoma
Opioids preoperatively • Short acting opioids • Study by Geller et al., Journal of Arthroplasty 2019: • Retrospective cohort of 500+ patients undergoing total joint arthroplasty • Looked at oxycodone given preop versus no opioid • Oxycodone patients had higher pain scores on postop day 1, walked short distances, and consumed greater morphine mg equivalents • One of many examples indicated that short acting opioids may be contributing to post-operative hyperalgesia • Methadone • Potent mu opioid receptor agonist with rapid onset and long duration of action • N-methyl-D-aspartate (NMDA) receptor antagonist
Intraoperative Components of ERAS • Normothermia • Euvolemia • Medications • Ketamine • Lidocaine • +/- Iv acetaminophen • Toradol • Dexamethasone • Dexmedetomidine • Esmolol • Type of anesthesia: spinal versus general anesthesia • Blocks or catheters post-induction or in OR prior to emergence
Intraoperative Components of ERAS (continued) • Euvolemia—Fluid management • Open incisions • Colorectal/abdominal surgery • Thoracic surgery • Laparoscopic • More liberal (although use caution in case of converting to open)
Intraoperative Components of ERAS (continued) • Medications : Ketamine • Pcp analog/dissociative anesthetic • Also has analgesic properties • Works mu opioid receptors and NMDA receptors • Intraoperatively: iv infusion or iv bolus • Postoperative: low dose iv infusion • Indications: • Severe postoperative pain expected (thoracic/abdominal/spine) • Opioid tolerant/dependent patients • Obstructive sleep apnea patients • Treats acute & chronic pain, decreases postoperative nausea & vomiting perioperatively
Intraoperative Components of ERAS (continued) • Lidocaine • Amide local anesthetic • potent anti-inflammatory, anti-hyperalgesic, and gastrointestinal pro-peristaltic drug. • Iv infusion or iv boluses • Level 1 evidence from gastrointestinal surgery demonstrates decreased pain scores, opioid analgesic consumption, and side-effects • Used as component of ERAS for many surgeries, most notably spines • Good for treating hyperalgesia or when opioids are not effective in treating acute pain
Intraoperative Components of ERAS (continued) • +/- IV acetaminophen • Toradol • NSAID given iv • Great for postoperative if given at end of surgery • Mixed evidence on postoperative bleeding • Concern but little evidence on delayed bone healing (spine) • Dexamethasone • Iv steroid • Treats postoperative nausea and vomiting • Treats pain • Prolongs regional blocks
Intraoperative Components of ERAS (continued) • Dexmedetomidine • alpha-2 adrenergic receptor agonist sedative, analgesic, and anti-sympathetic effects • adjuvant analgesic at all perioperative stages • potential adverse effects: sedation, hypotension and bradycardia • Esmolol • Given instead of opioids or to supplement opioids/reduce use • Shown to decrease postoperative pain intensity, opioid consumption, and postoperative nausea and vomiting
Postoperative Components of ERAS • Normothermia • Postoperative blocks or catheters • Consider same medications as preoperative • Muscle relaxants for muscle spasm (and anxiety) • PACU: iv diazepam (Valium) • Ketamine infusion • At UAMS can infuse on med/surg, followed by acute pain service • Lidocaine patch • Don’t discount effectiveness
Thoracic & Abdominal Epidurals for postoperative pain • Advantages • Great coverage for large incisions • Block sympathetic response to surgery • Facilitates earlier mobilization postoperatively & recovery of gut function • Reduces pulmonary, cardiovascular, thromboembolic, and gastrointestinal complications occurring after surgery • Disadvantages • Can be difficult to place in some patients • Requires close follow up & quick availability of anesthesia staff • Requires collaboration of multiple hospital services & Teams • Must monitor for and limit postoperative anticoagulation
Peripheral Nerve Blocks/CathetersUltrasound Guided • Benefits • Done preoperatively: • Improved hemodynamics • Decreased postoperative nausea and vomiting • Decreases postoperative opioid consumption • Risks • Small but present • Injury to nerve or surrounding structure • Infection • Bleeding • Reaction to local anesthetic • Allergy • Local anesthetic systemic toxicity
Peripheral Nerve Blocks/Catheters Single shot nerve block Peri-neural catheter Advantages Greater control over duration of block Can bolus or add adjuncts Can turn on/off pump for neural checks, physical therapy, etc. Disadvantages More training More thought More follow up Slightly more risk • Advantages • Fast, easy for most anesthesiologists to perform • Low maintenance • Little to no follow up • Disadvantages • Limited duration of block • Possibility of rebound pain
Exparel: liposomal bupivacaine • Lipids separating aqueous honey-comb shaped compartments, each containing bupivacaine • Slow release of bupivacaine • Slower onset of active than plain bupivacaine • Can be given with plain bupivacaine at time of injection • No additional local anesthetics should be given for 96 hours • Evidence for efficacy in literature depending on type of block and surgery • No evidence for improvement of pain peri-articular injections • Expensive
Peripheral Nerve Blocks/Catheters Upper extremity Lower extremity Chest wall & abdominal wall Brachial plexus blocks Block nerves individually Femoral Nerve Sciatic Nerve Ankle Chest Wall Intercostal Erector spinae Paravertebral Abdominal Wall Transverse abdominal plane Quadratus lumborum
Upper extremity blocksBrachial plexus anatomy • Nerve Roots • Interscalene • Trunks/Divisions • Supraclavicular • Cords • Infraclavicular • Branches • Axillary
Lower extremity blocksTwo main nerve component Femoral Nerve & Branches Sciatic Nerve & Branches Subgluteal nerve block Blocks entire sciatic nerve and branches Knee replacements, amputations Popliteal nerve block Tibial nerve Common peroneal nerve Below knee & ankle surgeries • Femoral nerve block • Block at level of groin • Hip fractures, hip replacements • Some knee surgeries • Femur involvement • Adductor canal • Mid-thigh • Saphenous nerve block • Minimal muscular component • Knee replacements, lower extremity
Chest wall blocks • Intercostal blocks • Usually performed by surgeons at end of surgery • May use Exparel (disadvantage—burns the bridge for other blocks) • Paravertebral • Similar to epidural block, have same constraints with anticoagulation • Erector spinae blocks • Deposit local anesthetic in plane deep to the erector spinae muscles and superficial to the transverse processes • Achieve a craniocaudal distribution along several vertebral levels. • Consider superficial block, less constraints with anticoagulation • Great for rib fractures, thoracotomies, back surgeries and some abdominal surgeries • May have local anesthetic spread to paravertebral & epidural spaces
Abdominal wall blocks • Transverse abdominal plane • Inject local anesthetic at the fascial plane between internal oblique muscle & transverse abdominis muscle • Limited to somatic anesthesia of the abdominal wall and highly dependent on interfascialspread • Will not help with visceral pain • Used for big abdominal incisions (with catheters) when epidural analgesia is not used • Quadratus lumborum • Somatic as well as visceral analgesia of both the abdominal wall and the lower segments of the thoracic wall • Provide visceral analgesia due to their paravertebral and possibly epidural spread
Summary of ERAS—putting it all togetherMultiple approaches to controlling pain at all stages of surgery Brain/Spine Peripheral Nerve Surgical site Acetaminophen NMDA antagonists Methadone Gabapentin Ketamine Alpha-2 agonists Dexmedetomidine Local anesthetics For neuroaxial analgesia Opioids work here but we want to minimize these Local anesthetics Peripheral nerve blocks/catheters Steroids Dexamethasone Alpha-2 agonists Local anesthetics NSAIDS Muscle relaxants
References • Deyo MD MPH, et al. Association Between Initial Opioid Prescribing Patterns and Subsequent Long-term Use Among Opioid-Naïve Patients: A Statewide Retrospective Cohort Study. J of Gen Intern Med. 2016: 32(1):21-7. • Cooper MD, et al. Preemptive Analgesia With Oxycodone Is Associated With More Pain Following Total Joint Arthroplasty. Journal of Arthroplasty. 2018: xxx 1-6. • SchwenkMD, et al. Consensus Guidelines on the Use of Intravenous Ketamine Infusions for Acute Pain Management From the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists. RegAnesth Pain Med. 2018; 43: 456-466. • N Eipe MBBS MD1, S Gupta MD, and J Penning MD. Intravenous lidocaine for acute pain: an evidence-based clinical update. BJA Education. 2016, 16 (9): 292–298. • Watts, et al. The effect of perioperative esmolol on early postoperative pain: A systematic review and meta-analysis.J AnaesthesiolClinPharmacol. 2017 Jan-Mar; 33(1): 28–39. • Chaoliang Tang and ZhongyuanXia. Dexmedetomidine in perioperative acute pain management: a non-opioid adjuvant analgesic. J Pain Res. 2017; 10: 1899–1904. • Nysora website: www.nysora.com/regional-anesthesia-for-specific-surgical-procedures