Download
1 / 39
460 likes | 724 Views
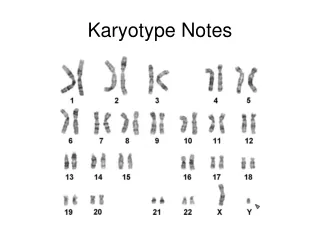
Molecular newbies in normal karyotype AML. Dr Hang Quach Haematology Registrar Box Hill Hospital. AML prognostic groups. Karyotype at diagnosis = independent prognostication Good prognostic group 70% 5 years OS .t(8;21)(q22;22)AML1-ETO Inv(16)MYH11-IgH .t(15;17)(q22;q21)PML-RARa

E N D
Molecular newbies in normal karyotype AML Dr Hang Quach Haematology Registrar Box Hill Hospital
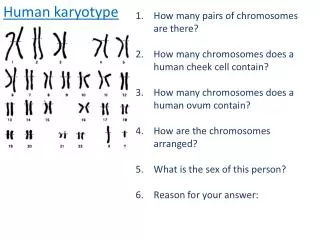
AML prognostic groups • Karyotype at diagnosis = independent prognostication • Good prognostic group70% 5 years OS • .t(8;21)(q22;22)AML1-ETO • Inv(16)MYH11-IgH • .t(15;17)(q22;q21)PML-RARa • Poor prognostic group<20% 5 year OS • -5,-7,abn(3q) or complex karyotype (>5abn) • Normal cytogenetics thought to be of intermediate prognosis: 30%-45% 5yr OS • ~50%
Normal karyotypic leukaemia – A heterogeneous group. • FMS tyrosine like kinase (FLT-3) • Nucleophosmin (NPM1) mutations • CAAT/enhancer binding protein alpha (CEBPalpha) • BAALC (brain and acute leukemia, cytoplasmic)
FLT-3 = STK1=flK2 • Class III receptor tyrosine kinase. • Structurally related to PDGFR, c-KIT • Human FLT3 gene = on chr 13q12 • Expression described on early hematopoietic and lymphoid precursors. • Imp role in stem cell survival + myeloid differentiation.
FLT3 mutations • Internal tandem duplications (FLT3 ITD) • Found in up to 30% of AML – mostly in normal karyotypes • Unfavourable prognosis (high relapse risk, decrease DFS and OS) • Point mutation in tyrosine kinase domain (FLT3-TKD) • 7% of AML • Point mutations and small deletions mostly of codons 835 and 836 • Thiede et al, Blood 2002: FLT3 mutation in 970pts • Both mutations were associated with similar clinical characteristics- higher WCC, higher blasts, monocytoid diff. • More prevalent in pt with normal karyotypes • Pt with high mutant/wt ratio (>0.78) worse OS and DFS
NucleophosminNPM1 NPM1 = nucleolar phosphosprotein. • A molecular chaperone: transport pre-ribosomal particles through nuclear membrane into cytoplasm. • Controls duplication of centrosomes during cell cycle • regulates tumour supressor pathway. • Mutated NPM1cytoplasmic translocation dimerises with wild type NPM 1cytoplasmic retention of NPM1.
Falini et al 2005 • 1835 paraffin embedded tumour specimen: • 591 = primary AML. • Pt were enrolled in italian trials: GIMEMA, LAM99P, GIMEMA/EORTC -M12. • 980 with extrahematopoietic neoplasms/hematopoietic malignancies other than “primary” AML. • Immunohistochemical detection of NPM1 localisation. • Using anti human monoclonal Ab against NPM1. • Correlation with clinical and biologic features of disease
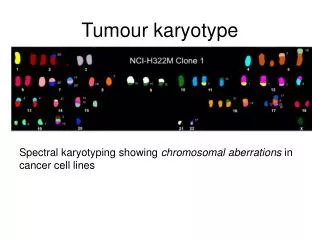
Method: Cont • Cytogenetics - G banding analysis. • RT-PCR for: • PML-RARa, AML-ETO, CBFb-MYH11, BCR-ABL. • FLT3 mutations.
Correlation with cytogentics Cytogentic data available for 493/591 pt with primary AML.
Co-expression of FLT-3 • FLT3 ITD found in 59/219 pt with normal karyotype (26.9%) • FLT-TKD (D835) found in 13/202 (6.4%). • FLT3 ITD was twice as frequent in the group with NPMc+ disease compared NPMc- disease, p<0.003 • Independent assocciation betweeen NPMc and FLT3 ITD on multivariate logistic regression model.
Blood Dec 2005, 106(12): 3773-39 • Retrospective analysis: • 401 AML pt with normal karyotype. • Age 16-81. • Entered AMLCG99 between 1999-2004. • Treatment: AMLCG study • Double induction: • TAD (Thioguanine, AraC, Daunorubicin)/ HAM (High dose araC, mitoxantrone) Vs HAM/HAM. • Consolidation -->radomised to maintenance for 3 yrs Vs AutoSCT.
Cytogenetics: G banding analysis. • Screening for NPM1 gene mutation using melting curve based light cycler assay. • Also screened for: • FLT 3-ITD, FLT3-TKD mutations
NPM1 mutation, morphology and other biologic markers. • 212/401 pt (52.9%) were HTZG for NPM1 mutation. • Higher expression in monocytic differentiation. • No sig difference with incidence of NPM1 mut b/w age groups. • Higher WCC in NPM1 mutation: • Mean 61.1 x10^9/L vs 39.1x10^9/L, p<0.001.
NPM1 mutations and other gene mutations. • NPM1-mutated groups showed significantly higher incidence of FLT3 mutations: • FLT ITD: 40.6%vs 24.5%, p=0.001 • FLT-TKD: 9.5%Vs 3.8%
Prognostic impact of NPM1 mutations. • 401pt • Median follow up=484d • CR was significantly higher in the NPM1 mutated cases: • 70.5% Vs 54%, p=0.003 • EFS: NPM mutated group:428d vs 336 days, p=0.012.
Median OS • Median OS in the NPM1 mutated group trends towards better prognosis: • 1012d vs 549d, p=0.076
Effects of additional FLT3 mutations Median OS: • NPM1+/FLT3-: 1183d • NPM1-/FLT3-: 601d • NPM1-/FLT3+: 401d • NMP1+/FLT3+: 321d
Event free survival • Same pattern was found with EFS: • NPM1+/FLT3-:773d • NPM1-/FLT3-: 365d • NPM1-/FLT3+: 279d • NMP1+/FLT3+: 234d
Relapse free survival. • RFS was significantly better for the NPM1+/FLT3- group compared to all other 3 groups, p= 0.001
Summary • NPM1 gene mutation occurred more frequently than any other muation in normal karyotypic AML: ~53% in this study • Favourable impact on outcome: • Longer EFS (med 428 vs 336d,p=0.12) • Trend to longer OS (med 1012 vs 549d, p= 0.076) • Favourable impact of NPM1 mutation is lost with concomitant FLT3-ITD mutations.
CCAAT/enhancer binding protein(C/EBP) • A member of the leucine zipper transcription factor family-gene located on 19q13.1 • In human: genes recently isolated and shown to be preferentially expressed in myelomonocytic cells (not erythroid, T or B lineages) • Specifically up regulated during granulocyte differentiation. • Regulates promoters of granulocyte specific genes.
C/EBP deficient mice lacked mature granulocytes(zhang et al proc Natl Acad Sci USA, 1997) • C/EBP mutations found in 7% of AML (Gombart eg al, Blood 2002) • Mutation resulted in a truncated C/EBP protein. • Inhibits wild type C/EBPa DNA binding. • Frequency was highest in those with FAB subtype M2, the majority of whom had normal cytogenetics. • In pt with t(8;21)AML1-ETO fusion protein down regulates CEBPa expression to a level insufficient for granulocyte differentiationAML-M2
Objective: • assess the prognostic relevance of CEBPA mutations in young adults with normal karyotypic AML • Search for cooperating mutations. • Diagnostic BM or PB samples from 236 pts (16-60yo) with normal cytogenetics: • 72pts: AML HD93 (1993-1998): • 164pts: AMLHD98(1998-2002) • Treatment: • Double induction: ICE x 2 (Ida 12mg/m2 d1,3,5; AraC100mg/m2 d1-7, Etop 100mg/m2 d1-3) • consolidation with HAM (AraC3g/m2bd d1-3, mitox 12mg/m2 d2,3) • 2nd consolidation: HD93: HAM; HD98: HAM or autoSCT.
Method • Cytogenetics – G banding analysis • FISH for other common AML-associated aberrations. • Analysis of CEBP coding regions: • amplified by PCR, abn products clonedSequenced the entire coding regions. • Other mutations also assessed: • FLT3 ITD, FLT3-TKD • MLL PTD
Results: • 36/236 (15%) pt demonstrated at least one CEBPa mutation • FLT3 mutations were significantly less freqent in pt with CEBP mutations: 28% v 49%, p=0.01 • None of the pts with CEBP mutation had MLL PTD.
Response to induction • Rates of CR (standard criteria) and resistant disease were not significantly different in patients with or without CEBP mutations, p=0.17
Remission duration • Median follow up 30 months • Median duration of remission: • 26 months in those without CEBP mutation. • Not reached for group with CEBP • P=0.01 Remision duration
Overall survival • OS longer for patients with CEBP mutations compared to wild type. • P=0.05 Overall survival
Multivariate analysis - OS CEBPA – an independent prognostic marker affecting remission duration and OS
Effects of additional FLT3 mutation • Among 36 pt with CEBPA mutation, presence of FLT 3 mutation (both ITD and D835) did not significantly influence OS, p=0.71
Summary - CEBP • CEBPA mutations detected in 15% of pts with normal karyotype AML. • CEBPA = an independent favourable prognostic marker on multivariate analysis (remission duration and OS) • Presence of FLT3 mutations had no -ve impact on pt with CEBPA mutations. • (not consistent with other studies)
BAALC (Brain and acute leukaemia, cytoplasmic) • Recently identified gene -chr 8q22.3 • Encodes a protein of yet unknown function. • In hematopoietic cells: BAALC expression restricted to progenitor cells.
BAALC • BAALC expression found in AML and CML in blast crisis, but not in CML in chronic phase. (Tanner et al, Proc Natl Acad, Sci USA 2001:) • In AML with normal cytogenetics, high mRNA expression of BAALC seem to predict poor prognosis (baldus et al, Blod 2003) • High BAALC expression: (Baldus et al, JCO 2006) • Predictive of resistant disease • Higher cumulative incidence of relaspe • Inferior overall survival.