Download
1 / 25
250 likes | 439 Views
KLINIKA ANESTÉZIOLÓGIE A INTENZÍVNEJ MEDICÍNY LF UPJŠ A FNLP KOŠICE. Water balance, infusions. MUDr. Štefan Trenkler, PhD. I. KAIM UPJS LF a UNLP Košice. Košice 2012. Distribution of body fluids and the Na & K concentrations in the body water compartments.

E N D
KLINIKA ANESTÉZIOLÓGIE A INTENZÍVNEJ MEDICÍNY LF UPJŠ A FNLP KOŠICE Water balance, infusions MUDr. Štefan Trenkler, PhD. I. KAIM UPJS LF a UNLP Košice Košice 2012
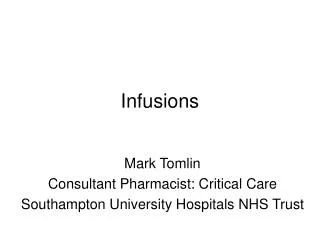
Distribution of body fluids and the Na & K concentrations in the body watercompartments 42 l = 28 + 14 (3,5 + 10,5) litres Lobo DN: Physiological Aspects of Fluid and Electrolyte Balance, 2002
Water, electrolytes homeostasis • Adequate volume of circulating plasma = normal tissue perfusion • ECF volume ~ total body Na+ content • Kidney – filtration, reabsorbtion of water, Na+ • Hormones – renin, aldosteron, ADH; ANP • Potassium
Na+: 1,5 mmol/kg/d K+: 1 mmol/kg/d
Homeostasis disturbances • Water – hyper and dehydratation • Osmolality (Na) – hyper a hypoosmolality • Oncotic disturbances • Ions disturbances • ABG disturbances
Osmotic pressure Osmotic pressure is force per area that prevents water from passing through membrane!
Fluid inputMaintaining the IC and EC fluid volume 1. Basic requirements (30 ml/kg/d)(1000 ml NS 0.9%; 2000 ml free water (Glu); 60 mmol KCl) 2. Pre-existing deficit (signs of dehydratation/hypovolemia - assessment) 3. Additional losses
Hydratation status, intravascular volume assessment • History • Physical examination (P, BP, RR, CR, MM, diuresis) • Tests results (Na, K, osmolality, HTC, urea) • Patient response to the fluid administration (physiological parameters)(10 – 20 ml NS 0.9%/kg)
Hypovolemia (fluid depletion) • Hypotension MAP<65 mm Hg, tachykardia • Diuresis • body weight • MAC (MLAC) • CVP • PAWP • LVEDP (TEE)
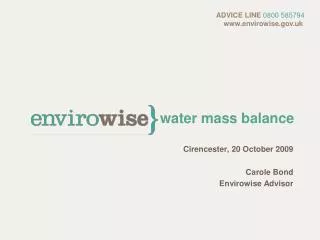
Distribution of infused fluids in the body water compartments Lobo DN: Physiological Aspects of Fluid and Electrolyte Balance, 2002
Natural Plasma 5 % (frozen) Albumin 4,5 %, 20 % Synthetic Gelatine Dextran 40, 70 Hydroxyetylstarch – HAES, Voluven, Colloids
Crystalloids vs colloids • No differences in clinical outcome • More oedema with crystalloids • More rapid replacement with colloids (permeability) • Risk vs benefit; cost • Newer (better) HEAS? • Mixture of C&C
Fluid replacement Loss of 1 liter of blood: Replacement: 1 l of blood or 1 l of colloid (IV) or4 l of crystalloid (EC) or12 l of glucose (IV + EC + IC) Distribution volumes of fluids! Speed of looses Replace what is lost Volume vs haemoglobin Oral/GI route has preference!!!
Guidelines for transfusion of red cellsAAGBI 2001 • Normally patients should not be not transfused if the haemoglobin concentration is >100 g/l. • A strong indication for transfusion is a haemoglobin concentration <70 g/l. • Transfusion will become essential when the haemoglobin concentration decreases to 50 g/l. • A haemoglobin concentration between 80 and 100 g/l is a safe level even for those patients with significant cardiorespiratory disease. • Symptomatic patients should be transfused
Transfusion trigger • HB (g/L) Clinical situation • 100 Acute coronary syndrome • 90 Stabile heart failure • 80 Aged, vascular surgery, sepsis • 70 All other patients
Blood transfusions • In the meantime –complex decision; prudent and conservative management, based on: - awareness of risks - individual haemoglobin level (70-100 g/L) - clinical judgement based on the sound understanding of the normaland pathological physiology - normovolaemia • Unit-by-unit basis (1 u ~15 g/l), re-evaluation • Departmental/hospital guidelines; regular audit • Haemovigilance system
Fluid regime • Preoperative deficits • Maintenance fluids • Blood loss • Losses to the third space
Situation • Blood volume: • 70 ml x 80 kg = 5600 ml • Blood loss: • 20% ~ 25-30 g/l = 90 g/l