Download
1 / 1
10 likes | 139 Views
Pure vascular dementia mimicking the behavioural variant of frontotemporal lobar degeneration : about 3 autopsied cases. V. Deramecourt 1, 2, 3 , F. Lebert 1, 2 , C.A. Maurage 1, 3, 4 , F. Pasquier 1, 2. 1 Univ. Lille Nord de France, EA1046, UDSL, Lille, France

E N D
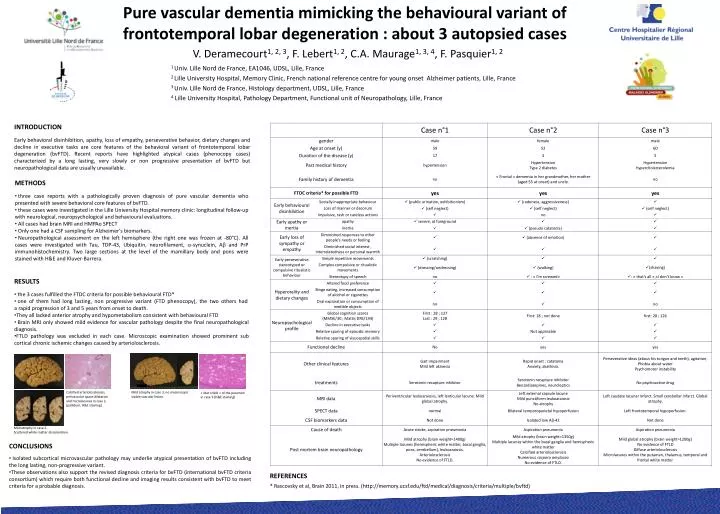
Pure vascular dementia mimicking the behavioural variant of frontotemporal lobar degeneration : about 3 autopsied cases V. Deramecourt1, 2, 3, F. Lebert1, 2, C.A. Maurage1, 3, 4, F. Pasquier1, 2 1 Univ. Lille Nord de France, EA1046, UDSL, Lille, France 2 Lille University Hospital, Memory Clinic, French national reference centre for young onset Alzheimer patients, Lille, France 3 Univ. Lille Nord de France, Histology department, UDSL, Lille, France 4 Lille University Hospital, Pathology Department, Functional unit of Neuropathology, Lille, France INTRODUCTION Early behavioral disinhibition, apathy, loss of empathy, perseverative behavior, dietary changes and decline in executive tasks are core features of the behavioral variant of frontotemporal lobar degeneration (bvFTD). Recent reports have highlighted atypical cases (phenocopy cases) characterized by a long lasting, very slowly or non progressive presentation of bvFTD but neuropathological data are usually unavailable. • METHODS • three case reports with a pathologically proven diagnosis of pure vascular dementia who presented with severe behavioral core features of bvFTD. • these cases were investigated in the Lille University Hospital memory clinic: longitudinal follow-up with neurological, neuropsychological and behavioural evaluations. • All cases had brain MRI and HMPAo SPECT • Only one had a CSF sampling for Alzheimer’s biomarkers. • Neuropathological assessment on the left hemisphere (the right one was frozen at -80°C). All cases were investigated with Tau, TDP-43, Ubiquitin, neurofilament, a-synuclein, Ab and PrP immunohistochemistry. Two large sections at the level of the mamillary body and pons were stained with H&E and Kluver-Barrera. • RESULTS • the 3 cases fulfilled the FTDC criteria for possible behavioural FTD* • one of them had long lasting, non progressive variant (FTD phenocopy), the two others had a rapid progression of 3 and 5 years from onset to death. • They all lacked anterior atrophy and hypometabolism consistent with behavioural FTD • Brain MRI only showed mild evidence for vascular pathology despite the final neuropathological diagnosis. • FTLD pathology was excluded in each case. Microscopic examination showed prominent sub cortical chronic ischemic changes caused by arteriolosclerosis. Calcified arteriolosclerosis, perivascular space dilatation and microlacunes in case 2. (pallidum, H&E staining) Mild atrophy in case 3, no macroscopic visible vascular lesion. « état criblé » of the putamen in case 3 (H&E staining) Mild atrophy in case 2. Scattered white matter discoloration. • CONCLUSIONS • Isolated subcortical microvascular pathology may underlie atypical presentation of bvFTD including the long lasting, non-progressive variant. • These observations also support the revised diagnosis criteria for bvFTD (international bvFTD criteria consortium) which require both functional decline and imaging results consistent with bvFTD to meet criteria for a probable diagnosis. REFERENCES * Rascovsky et al, Brain 2011, in press. (http://memory.ucsf.edu/ftd/medical/diagnosis/criteria/multiple/bvftd)