Download
1 / 38
520 likes | 1.47k Views
Gastric Cancer. Matt White AM Report April 19, 2010. Objectives. Epidemiology Clinical Presentation Diagnosis Staging Treatment Screening. Objectives. Epidemiology Clinical Presentation Diagnosis Staging Treatment Screening. Epidemiology. Incidence: 21,260 cases in 2007

E N D
Gastric Cancer Matt White AM Report April 19, 2010
Objectives • Epidemiology • Clinical Presentation • Diagnosis • Staging • Treatment • Screening
Objectives • Epidemiology • Clinical Presentation • Diagnosis • Staging • Treatment • Screening
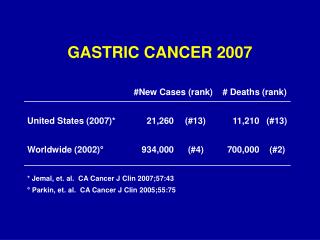
Epidemiology • Incidence: 21,260 cases in 2007 • ~7 per 100,000 • 11,210 cancer deaths in 2007 • Mortality significantly decreased in past 75 years (unknown reasons)
Gastric tumors • 85% adenoocarcinomas • 15% lymphomas and gastrointestinal stromal tumors (GIST)
Adenocarcinoma Cancer types • “Intestinal type” (more common) • Morphologically similar to intestinal adenocarcinomas. • Diffuse-type • Lack of intercellular adhesions (germline mutation in protein E-cadherin)
Spectrum of gastric cancer • Proposed progression: • chronic gastritis --> • chronic atrophic gastritis --> • intestinal metaplasia --> • dysplasia --> • adenocarcinoma
Risk Factors for gastric cancer • Diet • nitroso compounds • low fruit/vegetable, high fried foods/processed meat • High salt intake • Obesity • Smoking (HR 2-3) • ? Alcohol • H. Pylori • Low socioeconomic status • Hereditary diffuse gastric cancer • 40-67% lifetime risk for men, 60-83% for women • Immigrants from endemic areas • maintain native country risk, risk to offspring similar to new homeland
Objectives • Epidemiology • Clinical Presentation • Diagnosis • Staging • Treatment • Screening
Presentation • Approximately 50% of cases present with symptoms and have disease extending beyond locoregional confines • Of locoregional cases, only ½ can undergo a potentially curative resection
Symptoms (cont’d) • Dysphagia: more common with proximal gastric tumors • Occult GI bleeding very common, overt bleeding <20%.
Less Common Symptoms • Pseudoachalasia: if Auerbach’s plexus involved • Colonic obstruction: if cancer spreads (direct extension) to colonic wall
Signs • Palpable abdominal mass: most common physical finding • If cancer spreads via lymphatics… • Left supraclavicular node (Virchow’s) • Periumbilical node (Sister Mary Joseph) • Left axillary node (Irish) • Enlarged ovary (Krukenberg's tumor) • Ascites
Objectives • Epidemiology • Clinical Presentation • Diagnosis • Staging • Treatment • Screening
Diagnosis • EGD • Gold standard • Single biopsy from ulcer -> sensitivity ~ 70% • Seven biopsies from ulcer -> sensitivity >98% • Brush cytology increases sensitivity of single biopsies, aid in multiple biopsies unclear
Barium studies • False negative in as many as 50% of cases • Sensitivity as low as 14% in early cases • May be superior to EGD for linitis plastica • EGD may be normal while “leather-bottle” will be apparent on radiograph
Linitis Plastica • Diffuse-type gastric cancer • Tumor often infiltrates the submucosa and muscularis propria • Superficial biopsies may be falsely negative • Combination of strip and bite biopsy needed if suspicious for linitis plastica
Objectives • Epidemiology • Clinical Presentation • Diagnosis • Staging • Treatment • Screening
Staging of Gastric Cancer • Two systems: • Japanese classification (more elaborate and anatomic based) • Western: developed by American Joint Committee on Cancer (AJCC) and International Union Against Cancer (UICC) -- more widely used • Tumors at GE junction of in cardia of stomach within 5cm of GE junction • Classified using esophageal staging
Other caveats • T stage: dependent on depth of tumor invasion NOT size of lesion • Nodal stage: based on # of positive LN rather than location of LNs (proximity to tumor)
Staging workup • Biopsy • Imaging • CT: evaluates for metastases (M stage) • 20-30% with negative CT have intraperitoneal disease at laparatomy • Accuracy of 50-70% for T stage • Slightly worse accuracy for N stage compared to EUS • EUS: most reliable nonsurgical method to evaluate depth of invasion • More accurate than CT for T stage • 65-90% accurate for N stage
Staging workup • PET • More sensitive than CT for detection of distant metastases. • Also useful for detecting LNs • Negative PET not helpful- even large tumors can be falsely negative if metabolic activity low. • Most diffuse gastric cancers (signet ring) are not FDG avid
Staging workup • Serologic markers • CEA, CA-125, CA 19-9, CA 72-4 may be elevated but have low sensitivity/specificity • None are diagnostic • Preoperative elevation in markers usually pretends high risk of adverse outcome • No serologic finding should exclude surgical consideration
Objectives • Epidemiology • Clinical Presentation • Diagnosis • Staging • Treatment • Screening
Treatment • Locoregional (stage I-III) disease • Potentially curable • Refer for multidisciplinary evaluation and consideration of surgery • Advanced (stage IV) disease • Palliative therapy • Studies indicate longer survival and better quality of life with systemic treatment
Treatment • Complete surgical resection with removal of LNs (only chance of cure) • Possible in < 1/3 of cases • Subtotal gastrectomy for distal carcinomas, total or near-total for proximal masses • Reduction of tumor bulk (palliative) • Chemotherapy (cisplatin + 5-FU or irinotecan) • Partial response in 30-50% of patients • Radiation (for pain control, no mortality benefit with XRT alone)
Data from SEER. Patients diagnosed from 1991-2000 (n=14,097). Stage IA (n=1194), stage IB (n=655), stage IIA (n=1161) stage IIB (n=1195), stage IIIA (n=1031), stage IIIB (n=1660), stage IIIC (n=1053), stage IV (n=6148).
Prognosis ** Data from American Cancer Society
Objectives • Epidemiology • Clinical Presentation • Diagnosis • Staging • Treatment • Screening/Follow-up
Screening • Currently screening programs in Japan, Venezuela, Chile due to high incidence • Mostly barium studies, EGD is concerning findings • Some use serum pepsinogen testing for high risk with EGD confirmation • H. pylori: sensitivity 88%, specificity 41% (Japan) • Japan study: 5-year survival 74-80 in screened group, 46-56% for non-screened group. • Not cost effective in US due to relatively low incidence (<10 per 100,000) • Preventing incidence of 1 gastric cancer death estimated to cost $247,600
Gastric Ulcers • 25% of patient with gastric cancer have history of a gastric ulcer • American Society of Gastrointestinal Endoscopy recommendations: • Follow-up EGD in 8-12 weeks to verify healing. • Non-healing ulcers need repeat biopsies • Question of cost-effectiveness of repeat endoscopies; however, small (curable) lesions may be missed without follow-up.
Take Home Points • Most cases present in advanced stage • Staging workup (CT vs PET vs EUS) to evaluate extent of disease • Staging laparoscopy indicated for medically fit patients with >T1 lesion and without stage IV disease • Ensure follow-up of ulcers seen on EGD • No effective screening in US patients
References • Harrison’s Principles of Internal Medicine • Up to Date