Download
1 / 26
270 likes | 315 Views
L ESSON 1. Establishment of: The universally used coronary flow grading system to assess epicardial reperfusion, and demonstration of correlation between TIMI flow grade and survival in patients with STEMI

E N D
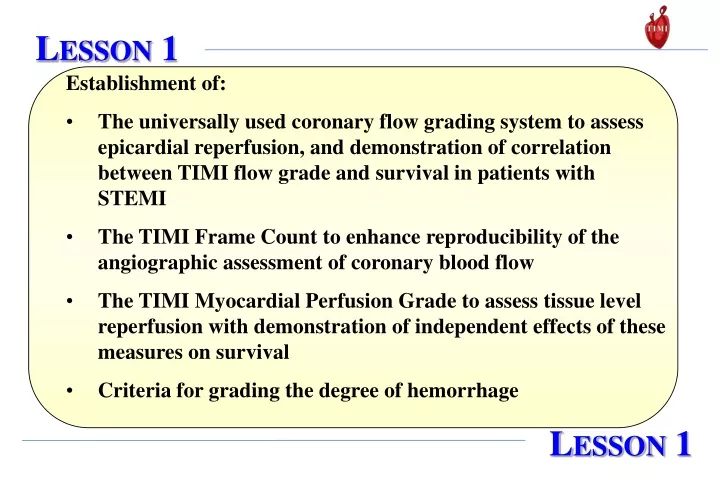
LESSON 1 • Establishment of: • The universally used coronary flow grading system to assess epicardial reperfusion, and demonstration of correlation between TIMI flow grade and survival in patients with STEMI • The TIMI Frame Count to enhance reproducibility of the angiographic assessment of coronary blood flow • The TIMI Myocardial Perfusion Grade to assess tissue level reperfusion with demonstration of independent effects of these measures on survival • Criteria for grading the degree of hemorrhage LESSON 1
LESSON 1 TIMI Flow Grade Mortality at 42 Days TIMI 0Complete occlusion TIMI 1Penetration of obstruction by contrast but no distal perfusion TIMI 2Perfusion of entire artery but delayed flow TIMI 3Full perfusion, normal flow P < 0.005 TIMI 1 Flygenring BP, J Am Coll Cardiol 1991;17:275A
LESSON 1 (Continued) Corrected TIMI Frame Count TIMI Grade 3 Flow Overall Mortality: 13% TIMI Grade 2 Flow Overall Mortality: 27% cTFC p = 0.015 TIMI 4 & 10 Gibson CM, Circulation. 1999;99:1945-50
LESSON 1 (Continued) Myocardial Perfusion Grade Epicardial TIMI Grade 3 Flow Overall Mortality: 3.7% Epicardial TIMI Grade 2/1/0 Overall Mortality: 7% 5 way p = 0.007 Myocardial Perfusion Grade 3 Myocardial Perfusion Grade 2 Myocardial Perfusion Grades 0/1 Myocardial Perfusion Grade 3 Myocardial Perfusion Grades 2/1/0 TIMI 10B Gibson CM, Circulation. 1999;99:1945-50
LESSON 1 (Continued) Major Hemorrhage: 1. Any intracranial or retroperitoneal bleeding 2. Clinically overt bleeding associated with a drop in Hgb of > 5g/dL (or absolute drop in Hct of 15%). A transfusion is counted as 1 g/dL or 3% Hct. Minor Bleeding: Clinically overt bleeding associated with a drop in Hgb of 3 to 5g/dL (or absolute drop in Hct of 9 to < 15%) and does not meet criteria for major hemorrhage TIMI 2 Bovill EG, Ann Intern Med 1991;115:256-65
LESSON 2 The first demonstration of the superiority of tissue plasminogen activator over streptokinase in the successful reperfusion of occluded coronary arteries in patients with STEMI. LESSON 2
80 t-PA * * 70 60 SK 62 % of Patients 40 43 *P<0.001 31 20 0 Reperfusion of Patency at 90 minutes occluded arteries LESSON 2 TIMI 1 TIMI Study Group, N Engl J Med 1985;312:932-36
LESSON 3 Demonstration of the superior efficacy of enoxaparin over unfractionated heparin in patients with unstable angina or non-ST elevation MI. LESSON 3
LESSON 3 Death/MI/Urgent Revascularization at 14 Days 20 UFH 16.7 % 18 ENOX 14.5 % 16 14 % 14.2 % 12 12.4 % 10 P=0.048RRR 15 % P=0.029RRR 15 % 8 6 4 2 0 2 4 6 8 10 12 14 Days TIMI 11B Antman EM, Circulation 1999;100:1593-1601
LESSON 4 Demonstration that simple risk scores (TIMI Risk Scores for UA/NSTEMI and STEMI) derived from baseline clinical information are powerful predictors of clinical outcomes and can improve therapy in patients with UA, NSTEMI, and STEMI. LESSON 4
LESSON 4 • One Point for each of: • Age > 65 y • > 3 CAD Risk Factors • Prior Stenosis > 50 % • ST deviation • > 2 Anginal events < 24 h • ASA in last 7 days • Elevated Cardiac Markers TIMI Risk Score for UA/NSTEMI % D/MI/Urgent Revascularization Vs TRS TIMI 11B Antman EM, JAMA 2000;284:835-842
LESSON 4 (Continued) Historical Age 65-74 2pts >75 3pts DM/HTN/Angina 1pt Exam SBP < 100 mmHg 3pts HR > 100 bpm 2pts Killip II – IV 2pts Weight < 67 kg 1 pt Presentation Anterior STE or LBBB 1 pt Time to Rx > 4hr 1pt ------------------------------------ Risk Score = Total (0-14) TIMI Risk Score for STEMI Mortality at 30 d vs. STEMI TRS TIMI 17 Morrow DA, Circulation 2000;102:2031-7
LESSON 4 (Continued) Simple Risk Score for STEMI Simple Risk Score Heart Rate x [Age/10]2 SBP Mortality (%) 30-day mortality by 43% for every 5 point in risk score Quartile Q1 Q2 Q3 Q4 Q5 Range <12.5 12.5–17.5 17.5–22.5 22.5–30 >30 TIMI 17 Morrow DA, Lancet 2001;358:1571-5 P< 0.0001 P< 0.0001 P< 0.0001
LESSON 5 Demonstration that an early invasive strategy results in improved clinical outcomes for patients presenting with UA/NSTEMI treated with GP IIb/IIIa inhibitor. LESSON 5
20 16 % Patients 12 8 4 0 0 1 2 3 4 5 6 Time (months) LESSON 5 Death, MI, Rehosp for ACS at 6 Months 19.4% 15.9% O.R 0.78 95% CI (0.62, 0.97) p=0.025 CONS INV Cannon CP, N Engl J Med 2001;344:1879-87 TACTICS-TIMI 18
LESSON 5 Death, MI, Rehosp for ACS at 6 Months CONS INV * OR=0.55 *p<0.001 Interaction P=0.013 p=NS (%) N= 426 414 480 506 TnT cut point = 0.01 ng/ml (54% of Pts TnT +) Morrow DA, JAMA 2001;286:2405-12 TACTICS-TIMI 18
LESSON 6 Demonstration that with a multimarker approach, troponin, hs-CRP, and BNP provide independent and complementary prognostic information in patients with UA/NSTEMI. LESSON 6
0.2 0.5 1.0 2 5 LESSON 6 Assign patients 1 point for the presence of each elevated biomarker (TnI > 0.1 ng/ml, CRP > 1.5 mg/dl, BNP > 80 pg/ml). RR of D/MI/CHF at 6 months OR & 95% CI for D/MI/CHF by 6 months Age (per year) Diabetes Prior MI Prior CHF ST deviation 0 Biomarkers 1 Biomarker 2 Biomarkers 3 Biomarkers Sabatine MS, Circulation 2002;105:1760-3 TACTICS-TIMI 18
LESSON 7 Demonstration that patients recently hospitalized for an acute coronary syndrome benefit from early, aggressive, and continued lowering of LDL-C to levels substantially below current target levels. LESSON 7
LESSON 7 DEATH, NON-FATAL MI, OR URGENT REVASCULARIZATION 20 Pravastatin 40 mg 15 16.7% Percent patients with events Atorvastatin 80 mg 10 12.9% RRR 25% 5 P=0.0004 0 0 6 12 18 24 30 Months of Follow-up Cannon CP, N Engl J Med 2004;350:1495-1504 PROVE IT-TIMI 22
LESSON 8 Demonstration that atorvastatin 80 mg results in a greater depression of C-reactive protein than pravastatin 40 mg, independent of LDL-C reduction, indicating that the anti-inflammatory actions of statins are of critical importance in reducing clinical events. LESSON 8
Pravastatin 40mg (n=1873) Atorvastatin 80mg (n=1872) P value Randomization 12 mg/L 12 mg/L 0.6 30 days 2.4 mg/L 1.7 mg/L <0.001 120 days 2.0 mg/L 1.3 mg/L <0.001 Study end 2.1 mg/L 1.3 mg/L <0.001 LESSON 8 C-reactive protein (hsCRP) levels by treatment Risk of Death or MI after Day 30 P=0.005 for prava P=0.6 for atorva PROVE IT-TIMI 22 Ridker PM, JACC 2005;45:1644-1648
LESSON 9 Demonstration that the addition of clopidogrel improves infarct-related artery patency and reduces death and ischemic complications in STEMI patients receiving standard fibrinolytic therapy including aspirin. LESSON 9
LESSON 9 Occluded Artery (or D/MI thru Angio/HD) Odds Ratio 0.64(95% CI 0.53-0.76) 36% Odds Reduction P=0.00000036 0.4 0.6 0.8 1.0 1.2 1.6 n=1752 n=1739 Clopidogrel better Placebo better Clopidogrel Placebo CLARITY – TIMI 28 Sabatine MS, N Engl J Med 2005;352:1179-89
LESSON 10 Demonstration that in patients receiving fibrinolysis for STEMI, a strategy of enoxaparin throughout the index hospitalization is superior to treatment with unfractionated heparin for 48 hours for preventing death or reinfarction but there is an increase in major bleeding. Net clinical benefit is significantly improved with the enoxaparin strategy. LESSON 10
LESSON 10 Main Secondary Endpoint: Death, non-fatal re-MI, urgent revascularization by 30 days Primary Endpoint: Death or non-fatal re-MI by 30 days UFH 14.5 UFH 12.0 11.7 9.9 ENOX ENOX % % RR = 0.83 p = 0.000003 RR = 0.81 p = 0.000001 Days Days Antman E, N Engl J Med 2006; 354:1477-88 ExTRACT-TIMI 25