Download
1 / 58
580 likes | 898 Views
Possible Applications of Triune Brain Theory in Developmental Disorders. Dr Khalid Mansour Locum Consultant Forensic Psychiatrist in Learning Disabilities Eric Shepherd Unit . How does the brain work?. Main functional structure of the brain? Brain centres (Phrenology) (too simple)

E N D
Possible Applications of Triune Brain Theory in Developmental Disorders Dr Khalid Mansour Locum Consultant Forensic Psychiatrist in Learning Disabilities Eric Shepherd Unit
How does the brain work? • Main functional structure of the brain? • Brain centres (Phrenology) (too simple) • Brain circuits (e.g. Papez circuit – FLS vs OPD – M R diffusion tensor imaging – Tractography) (vague, little clinical applications) • Evolutional/developmental approach (Triune Theory): • Strong scientific evidence • More comprehensive theory of brain functioning • High clinical potential
Triune Theory • “The most influential idea in neuroscience since World War II” (Durant in Harrington 1992) • MacLean’s Triune Brain Concept has had limited acceptance or been largely ignored by professional neurobiologist (Science Journal 1990 & American Scientist journals 1992) (Cory in Cory & Gardner 2002)
(I) Triune theory Senior Research Scientist National Institute of Mental health 1913 - 2007
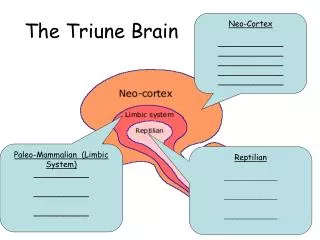
Triune Theory Vertebrates can be divided from evolutionary point of view into three main categories: • Animal with brains made mainly of spinal cord, brain stem, basal ganglia and cerebellum (reptilian brain, the R-Complex or the Striatal Complex): e.g. Reptiles, birds & fish • Animals which brain is mainly made from the R-Complex + the limbic Lobe (diencephalons, Amygdala, septum, Mammillary body, Fornix, limbic cortex: Broca’s area, cingulated cortex, hippocampus & others): e.g. Rats, cats , dogs and monkeys • Animals which brain is mainly made of: R-Complex + Limbic System + the Neocortex: e.g. Apes and humans
Triune Theory (I) Animal with brains made mainly of Reptilian brain(R-Complex) • Mainly Reptiles, birds & fish • Evolutionary functions: • Motor behaviour including motor routines, motor subroutine, motor memory and motor (non-verbal) communications • Primitive emotions: rage, fear & submissiveness • Copulation
Triune Theory (II) Animals which brain is mainly made from the reptilian brains + the limbic Lobe: • Lower mammals e.g. Rats, cats , dogs and monkeys • Evolutionary functions: (beginning of family) • Nursing of the offspring (parental care) • Vocalisation (audio-vocal communication) • Play
Triune Theory (III) Animals which brain is mainly made of: R-Complex + Limbic System + the Neocortex: • Higher mammals e.g. Apes and humans • Evolutionary functions: (beginning of cultures) • Problem solving skills (Mentation) • Learning • Detailed memory • Verbal communication • Preservation of ideas
Clinical Applications of the Triune Theory in Developmental Disorders: • Triune Brain > Triune “Intelligence” • Better clinical assessment and diagnosis of autism • Better diagnostic criteria of Autism • Better understanding of aetiology of ASD • Schizophrenia and Autism
(1)Triune Brain: Triune Intelligence • R-Complex: processing object related data > Object-Related Skills / Intelligence • Limbic System: processing emotional data > Emotional Skills / Intelligence • Neocortex: processing social data> Social Skills / Intelligence • We could have : • Object related intelligence (general intelligence - IQ), • Emotional Intelligence & • Social intelligence
(1)Triune Brain: Triune Intelligence • Object Related Intelligence (general intelligence - IQ): managing physical environment (not emotionalised – not socialised) e.g. budgeting and travelling • Emotional Intelligence: managing emotional/personalised environment e.g. emotional bonding, insight and empathy. • Social Intelligence: managing social environment e.g. functioning in social groups and social appropriateness.
(1)Triune Brain: Triune Intelligence Why Three-Dimensional Intelligence? • Clinical Evidence: Emotional Intelligence and Social Intelligence, are used in every day clinical work • Emotional intelligence: (Leuner,1966; Payne, 1985; Greenspan, 1989; Salovey and Mayer,1990; Goleman, 1995). • Social Intelligence: (Cohen, 2000; Goleman, 2006) • ASD: a good example of the separation of Object Related Intelligence from Emotional Intelligence and Social Intelligence
(1)Triune Brain: Triune Intelligence Potential applications of triune intelligence: • Explains variations in development of intelligence • One step towards more use of IQ format • Object related intelligence (General intelligence) IQ • Emotional intelligence IQ • Social Intelligence IQ • End of categorical classification of ASD
(2) Better diagnostic criteria of Autism Current Diagnostic Criteria DSM-IV (I) A total of six (or more) items from (a), (b), and (c), with at least two from (a), and one each from (b) and (c) (A) qualitative impairment in social interaction: • impairments in nonverbal behaviors such as eye-to-eye gaze • failure to develop peer relationships • lack of spontaneous seeking to share enjoyment, interests, or achievements • lack of social or emotional reciprocity (B)qualitative impairments in communication: • delay in the development of spoken language • marked impairment in sustain a conversation • idiosyncratic language • lack of social imitative play
(2) Better diagnostic criteria of Autism Current Diagnostic Criteria DSM-IV (cont) (C)Restricted repetitive and stereotyped patterns of behavior, interests and activities: • stereotyped and restricted patterns of interest • inflexible nonfunctional routines or rituals • stereotyped and repetitive motor mannerisms • preoccupation with parts of objects (II) Delays with onset prior to age 3 years: (III) The disturbance is not better accounted for by Rett's Disorder or Childhood Disintegrative Disorder
(2) Better diagnostic criteria of Autism Proposed Diagnostic Criteria (1) Essential features: • Poor development of social intelligence/skills • Lack of social reciprocity • dysfunctional social aspects of play • dysfunctional social aspects of communication • Social awkwardness • failure to develop peer relationships • Poor development of emotional intelligence/skills : • Self-centredness with poor self awareness • lacking empathy (dysfunctional theory of mind) • Lack of emotional reciprocity • Poor appreciation of emotional expressions • Emotional awkwardness • Poor emotional aspects of play • Poor emotional aspects of communication
(2) Better diagnostic criteria of Autism Proposed Diagnostic Criteria (Cont) (2) Compensatory Features: (Try to feel less overwhelmed, more in control and more secure): • Restricting environment • Restricting interest • Islets of exceptional interests • tendency to keep rigid control over environment • Rigid routines or rituals (3) Associated features: • Existential (not stress related) anxiety • Pathological habits (dysfunctional routines) • Poor development of speech • Poor eye to eye contact • OCD like symptoms and rituals • Motor mannerisms • Preoccupations with parts of objects
(3) Better clinical assessment of Autism • Autism is primarily a disorder of emotional and social development which could be due to developmental abnormalities in both limbic system and neocortex. R-Complex could be intact or affected too. • All affected brain functions could take different forms: • lost functions (like in ablation studies) • exaggerated functions (irritation or excitation studies) • partially lost or partially exaggerated • Assessment of each neurological part separately: • Assessment of R-Complex • Assessment of Limbic System • Assessment of Neocortical System
(3) Better clinical assessment of Autism General assessment of R-complex • General functioning • Deals mainly with objects related data • Function: survival in physical world • Produce behavioural routines • Specific functioning • Routines (skills), • Habits, • Motor Communication, • Repetitions (OCD like symptoms) • Assessment of the subsystem • Arousal or motivation assessment (e.g. rocking, ADHD) • Involuntary muscular movements
(3) Better clinical assessment of Autism Development of motor routines
(3) Better clinical assessment of Autism R-Complex Specific Functioning • Object related Routines: functional motor routines • Primitive e.g., territorial behaviour • Advanced e.g. tidying one’s room • Object-related Habits (Pathological) : not functional motor routines e.g. pica, addiction, fire setting • Object-related Checking (repetitive) behaviour: e.g. • Exaggerated routines (e.g. hoarding) • Failed to execute routines (repetitive behaviour or OCD like symptoms)
(3) Better clinical assessment of Autism General assessment of Limbic System • General functioning • deals mainly with emotional (individual-related) data • Function: survival in the physical world as an individual • Not normally functional in autism • Specific functioning (emotional routines and habits) • Play • audio-vocal communication • Attachment with others • Theory of mind • Assessment of the subsystem • Attachment disorders
(3) Better clinical assessment of Autism Limbic System Specific functioning: • New emotional routines: not well developed in ASD e.g. • Self centeredness • Hostile dependence on safe relations • Increased anger or increased blaming behaviour, • Dysfunctional empathy • Pathological emotional habits e.g. • deviated sexual interests (paedophilia) • Dysfunctional emotional communication e.g. • “one way communication” “talking at you not to you” • Existential anxiety
(3) Better clinical assessment of Autism General assessment of Neocortical system • General functioning of Neocortex • Deals mainly with social (group) data • Function: survival in the physical world as anindividual who is in the same time a member of a bigger social group • Specific functioning • Social Routines (skills) • Social Habits (pathological) • Social Communication • Assessment of the subsystem • Imagination / Fantasy disorders (?)
(3) Better clinical assessment of Autism Neocortical System Specific functioning: • Social routines: how undeveloped • Failure of functions: social isolation, social awkwardness • Exaggerated functions: paranoid social attitudes (Nicky Reilly Syndrome) • Pathological habits: • Drug-misuse-to-fit-in syndrome, • hoax phone calls, • Pyromania • Social communication disorder • Poor appreciation of danger (naivety syndrome)
(4) Better understanding of aetiology of ASD • No single aetiology for ASD • Pathway of aetiologies • Upward connections from R-Complex to LS and/or to neocortex • Downward connection from Neocortex and/or LS to R-complex • Each connection can be disturbed by different mechanisms