Download
1 / 37
420 likes | 537 Views
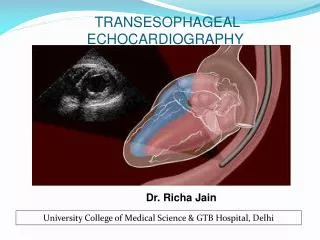
TRANSESOPHAGEAL ECHOCARDIOGRAPHY GOAL DIRECTED FLUID THERAPY DURING ANESTHESIA. Dr Piyush Mallick MD Consulatnt Anesthesia & ICU. Al Zahra Hospital Sharjah. INTRODUCTION. In 1976, Dr Leon Frazin - concept of TEE.

E N D
TRANSESOPHAGEAL ECHOCARDIOGRAPHYGOAL DIRECTED FLUID THERAPY DURING ANESTHESIA Dr Piyush Mallick MD Consulatnt Anesthesia & ICU Al Zahra Hospital Sharjah
INTRODUCTION • In 1976, Dr Leon Frazin - concept of TEE. • Echocardiography:- the heart and great vessels probed with ultrasound (sound with frequency above 20 kHz). • Echocardiography uses ultrasound waves with frequency of 2.5 – 7.5 MHz. • Ultrasound sent into thoracic cavity and partially reflected by cardiac structures. • From these reflections: distance, velocity and density of objects within the chest derived.
INDICATIONS FOR PERIOPERATIVE TEE • Preoperative: hemodynamically unstable patients with no definite diagnosis like suspected thoracic aortic aneurysms, dissection, or undifferentiated shock state • Intraoperative: • acute, persistent, and life-threatening hemodynamic disturbances • valve repair, CHD surgery for lesions requiring cardiopulmonary bypass; repair of hypertrophic obstructive cardiomyopathy; endocarditis; repair of aortic dissections; pericardial window procedures.
INDICATIONS FOR PERIOPERATIVE TEE • In ICU: unstable patients with unexplained hemodynamic disturbances, suspected valve disease, or thromboembolic problems. • TEE guided CPR in ED cardiac arrest ( Both for diagnosis & Monitoring whether effective CPR)
TEE EQUIPMENT • Monitor and TEE probe • TEE probe: a minaturized echocardiographic transducer (40mm long, 13mm wide and 11 mm thick) mounted on the tip of a gastroscpoe. • Transducer: a phased array configuration with 64 piezoelectric elements operating at 3.7 to 7.5 MHz. • 2 knobs: one controls anteflexion and retroflexion; other controls rightward and leftward movement of the probe. • One electronic switch to scan the heart in various axial views .
PROCEDURE • Induction of anaesthesia and tracheal intubation • Patient’s neck extended • Well lubricated TEE probe introduced into the midline of hypopharynx with transducer facing anteriorly • Probe advanced into esophagus • During this manoeuvre, the control knob must be in neutral position.
Terminology used to describe transesophageal echocardiography probe movements.
I III II I- UPPER ESOPHAGEAL II- MID ESOPHAGEAL III- TRANSGASTRIC
Transesophageal echocardiography cross sections in a comprehensive examination.
WHAT ANESTHESIOLOGIST SHOULD KNOW ? • EVALUATIONOFLVFILLING : • TEE reveals changes in left ventricular preload and filling pressure. • It measures EDA (end diastolic volume). EDA < 12cm2 - hypovolemia • Assessment of LV filling and function subjectively with the “trained eye”: a valid method to guide fluid administration.
CARDIAC OUT PUT WITH EACH BEAT 2. ESTIMATION OF CARDIAC OUTPUT: • Real-time TEE images of LV filling and ejection permits qualitative, immediate detection of extreme changes in cardiac output. • TEE quantify CO the velocity and the cross-sectional area of blood flow. • SV = v x ET x CSA SV = stroke volume (ml) v = spatial average velocity of blood flow (cm/sec) ET = systolic ejection time (sec) CSA = cross-sectional area of the vessel (cm2 )
SYSTOLIC & DIASTOLIC FUNCTION 3. Assessment of ventricular systolic function: • Fractional area change (FAC) during systole: a measure of global LV function. • FAC = EDA – ESA / EDA EDA : cross-sectional area at end diastole ESA : cross-sectional area at end systole. • Marked changes in FAC are apparent by simply viewing the real-time images. • Hallmarks of severe RV dysfunction: severe hypokinesis , enlargement of RV , change in shape of RV from crescent to round.
DIASTOLOGY FOR HFPEF 4. Assessment of ventricular diastolic function: • TEE is an ideal tool for assessment of diastolic function because of its unobstructed view of the mitral valve and pulmonary veins. • Normal flow across the mitral valve in diastole has • E wave : an early higher-velocity component (generated by atrial pressure and ventricular relaxation) • A wave : lower-velocity component (generated by atrial contraction) • At slower heart rates, these two waves are separated by a period of relatively little flow (diastasis).
TAPSE & S prime for RV function • Video
Line drawings representing simultaneous transesophageal pulsed wave Doppler recordings from the mitral annulus and right upper pulmonary vein.
HOW MUCH FLUID ?HOW MUCH IS TOO MUCH ?WHEN TO STOP? 1.Based on mitral valve study 2.Using E/A wave ratio 3. Tissue Doppler e/a ratio
WHAT HAPPENES IN MYOCARDIAL ISCHEMIA? 5. Detection of myocardial ischemia: • Acute myocardial ischaemia produce abnormal inward motion and thickening of affected myocardium. • Short axis view of LV at level of papillary muscle : best view • Wall thickening more specific marker than wall motion.
SVC COLLAPSIBILITY AND FLUID RESPONSIVENESS 20% TO 30 % COLLAPSIBILTY
ME bicaval IAS LA IVC SVC Eustachian valve Left Atrium (LA) Right Atrium (RA) Inferior Vena Cava (IVC) Superior Vena Cava (SVC) Intra atrial septum (IAS) Right Atrial Appendage Fossa Ovalis RA
CAN WE SEE PULMONARY EMBOLISIM ( BLOOD CLOT/GAS/AMNIOTIC FLUID) • RV bigger than LV • D shaped LV • McConnel sign • You can really see the clot
ME asc aortic SAX Rt PA SVC PA Asc Pulmonary Artery (PA) Right Pulmonary Artery (Rt PA) Superior Vena Cava (SVC) Ascending Aorta (Asc)
ME asc aortic LAX Orientation: Ascending Aorta (Asc) Right Pulmonary Artery (Rt PA) Rt PA Asc Proximal Distal
IMAGING TECHNIQUES • M MODE • One-dimensional views of cardiac structures produced by single-crystal transducers . • Density and position of all tissues in the path of a narrow ultrasound beam displayed as a scroll . • It is a timed motion display. • Principally used to view rapidly moving structures eg. valve leaflets. • Disadvantages: orientation and interpretation of spatial relationships difficult.
M-mode transesophageal echocardiogram of a normal aortic valve
IMAGING TECHNIQUES • 2D MODE • Rapid, repetitive scanning along many different radii within an area in the shape of a fan (sector). • A live (real time image) of heart is produced. • Advantage: the image obtained resembles an anatomic section and can be easily interpreted.
two-dimensional cross section of a normal aortic valve (AV)..
IMAGINGTECHNIQUES • DOPPLER TECHNIQUE:- • Based on doppler principle. • With doppler, blood flow velocity can be measured. • Different types of Doppler techniques: • Pulsed wave doppler • Continuous wave doppler • Colour flow doppler
BART • BLUE AWAY • RED TOWARDS
Different types of doppler technique TISSUE DOPPLER • A new use of PWD technology • To measure myocardial velocity. • It measures the velocity of the descent of the mitral annulus (Sm) towards the apex of the heart during normal LV contraction. • It decreases in presence of myocardial ischemia.
LA PRESSURE ESTIMATION • PCWP not needed for LA pressure estimation • Pulse wave doppler / Tissue doppler • Can diagnose impending Pulmonary Edema
DISADVANTAGES OF TEE • Semi invasive procedure : chances of injury • Needs special set up, technique, preparation, instrumentation • Needs orientation and expertise
CONTRAINDICATIONS OF TEE • ABSOLUTE: • Previous esophagectomy • Severe esophageal obstruction • Esophageal perforation • Ongoing esophageal haemorrhage • RELATIVE: • Esophageal diseases-diverticulum, varices, fistula • Previous esophageal surgery • Previous mediastinal irradiation • Unexplained swallowing difficulty
COMPLICATIONS OF TEE • Oral and pharyngeal injuries (0.1 – 0.3%) • Transient hoarseness (0.1 – 12%) • Esophageal injuries • Splenic injuries – 2 case reports • Endocarditis in outpatients