Download

1 / 35
350 likes | 468 Views
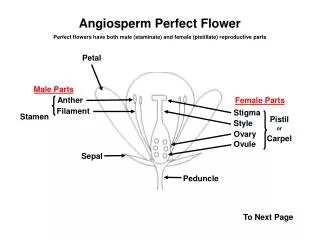
F.O.G.S.I. Fe & Female Workshop. Organised by Nashik Ob/Gy Society. Hazards of Blood Transfusion. Presented by Dr. Ravindra S. Shivde M.D.,D.G.O. MILESTONES:. Andreas Libavius- 1546-1616 James Blundell- 1818 Karl landsteiner- 1900. Blood Transfusion. General Tonic?.

E N D
F.O.G.S.I. Fe & Female Workshop Organised by Nashik Ob/Gy Society Hazards of Blood Transfusion Presented byDr. Ravindra S. ShivdeM.D.,D.G.O. Hazards of Blood Transfusion
MILESTONES: • Andreas Libavius- 1546-1616 • James Blundell- 1818 • Karl landsteiner- 1900 Hazards of Blood Transfusion
Blood Transfusion General Tonic? Hazards of Blood Transfusion
Risks of Blood Transfusion • Incompatible blood • Allergy, febrile reaction • Infection • Immunosuppression Immunosuppression Infection Noninfectious Hazards Hazards of Blood Transfusion
Risks of blood transfusion( Per unit of blood U.S.A. ) • Minor allergic reactions 1:100 • Viral hepatitis (A,B,C,D,G) 1:50,000 • Hemolytic reactions 1:6,000 • Fatal hemolytic reactions 1:600,000 • HIV infection 1:420,000* • HTLV-I/II 1:200,000 • Bacterial infections 1:2,500 • Acute lung injury 1:500,000 • Anaphylactic shock 1:500,000 • Graft Vs. host disease Rare • Immunosuppression 1:1 Hazards of Blood Transfusion
Transfusion-transmitted infections Post-transfusion purpura 3% Acute lung injury 6% 8% Graft vs host disease 2% Incorrect blood/ componenttransfused 14% 53% Delayed transfusion reaction 15% Acute transfusion reaction Based on 366 spontaneously-reporteddeaths/major complications between October 1996 and September 1998 in the UK and Ireland. Serious Hazards of Transfusion Williamson LM, et al. BMJ. 1999;319:16-9. Hazards of Blood Transfusion
Infectious complications • Viruses • HIV-1,2 … • HTLV-I,II • Cytomegalovirus • Epstein-Barr virus • Parvovirus B19 • Creutzfeldt-Jakob disease(CJD) • TTV • West Nile • Spirochetes • Treponema pallidum • Borrelia burgdorferi • Parasites • Plasmodia • Babesia microlti • Trypanosoma crizi • Toxoplasma gondii • Leishmania donovani • Bacteria • Staphylococcus • Salmonella • Yersinia enterocolitica Hazards of Blood Transfusion
Risks of Transfusion: Infectious Disease • HIV = 1 in 1.8 million • HCV = 1 in 1.6 million • HBV = 1 in 220,000 HIV = human immunodeficiency virus. HCV = hepatitis C virus. HBV = hepatitis B virus. Busch MP, et al. JAMA. 2003;289:959-62. Hazards of Blood Transfusion
Risks of Allogeneic Blood ‘TRIM’ Transfusion Related Immune Modulation Hazards of Blood Transfusion
Immune modulation • Allogeneic transfusion may enhance tumor recurrence following colorectal cancer resection (Heiss MM, J Clin Oncol 1994) • Allogeneic transfusion is associated with prolonged hospital stay (Vamvakas EC, Transfusion 2000) • Allogeneic transfusion is associated with increased risk of bacterial infection (35%) and pneumonia (52%) (Carson JL, Transfusion 1999) • Length of storage of transfused RBCs was associated with postoperative pneumonia following CABG surgery, 5% per unit (Vamvakas EC, Transfusion 1999) Hazards of Blood Transfusion
Immune Effects of Blood • Immunologic effects of autologous/allogenic blood Tx • Decreased T-cell proliferation • Decreased CD3, CD4, CD8 T-cells • Increased soluble cytokine receptor • sTNF-R, sIL-2R • Increased serum neopterin • Increased cell-mediated lympholysis • Increased TNF-alfa • Increased suppressor T-cell activity • Reduced natural killer cell activity Hazards of Blood Transfusion McAlister FA et al, Br J Surg 1998;85:171-8. Innerhofer P et al, Transfusion 1999;39:1089-96.
Blood Tx Increases Risk of Postoperative Bacterial Infection • 20 peer-reviewed studies, 1986-2000 • N = 13,152 (Tx 5215, No-Tx 7937) • Association of Blood Tx to Infection • Common OR 3.45 (range 1.43-15.15) • 17 of 20 studies with p < 0.05 • Trauma subgroup • Common OR 5.26 (range 5.03-5.43) • All studies with p < 0.05 (0.005 – 0.0001) • Blood Tx associated with greater risk in trauma pts Hill GE, Minei JP et al. J Trauma 2003;54:908-914 Hazards of Blood Transfusion
Nosocomial Infection Rates in Critically Ill Patients For each unit of PRBCs given, the odds of infection is increased by a factor of 1.5 P < .05 N = 1,717 n = 416 n = 1,301 Adjusted for severity of illness using MPM-0 scores, age, gender (Project IMPACT). Taylor RW et al, Crit Care Med 2002;30:2249-54. Hazards of Blood Transfusion
The Impact of PRBCs on Nosocomial Infection Rates in ICU • Retrospective database study of 1,717 patients using Project IMPACT • NI rates of 3 groups were compared: • Entire cohort • Transfusion group • Nontransfusion group • Patients stratified for age, gender, and probability of survival using Mortality Prediction Model (MPM-0) scores Taylor RW et al, Crit Care Med 2002;30:1-6. Hazards of Blood Transfusion
Do Blood TransfusionsImprove Outcomein Sepsis? Hazards of Blood Transfusion
Mortality Rates in Critically Ill Patients P < .05 N = 1,717 n = 416 n = 1,301 Taylor RW et al, Crit Care Med 2002;30:2249-54. Hazards of Blood Transfusion
TRALI • 1:2000 transfused patients • FDA reports as the third most prevalent transfusion related mortality, after hemolysis and sepsis • Associated with: whole blood, RBC, platelets, FFP and cryo. • CHF – ARDS, fleeting or devastating • Two prominent theories • HLA class I and possible II, and monocyte antigens • 20% of women with multiple gestations carry class I antigens • Mixture of predisposition and infusion of blood related lipid derived mediators Hazards of Blood Transfusion
Donor Leukocytes • Persistence of donor WBCs in trauma patients for up to 1.5 years after an allogeneic blood transfusion • ‘Survival of donor leukocyte subpopulations in immunocompetent transfusion recipients: frequent long-term microchimerism in severe trauma patients’ • 2 x 109 WBCs in one unit of packed red blood cells • 1 x 108 WBCs – centrifuged, buffy coat depleted • 1–5 x 106 WBCs – leukocyte filter, leukocyte-depleted Hazards of Blood Transfusion Lee TH et al, Blood 1999;93:3127–3139
Why is blood transfusionNOT associated withimproved outcome? Hazards of Blood Transfusion
Age of Blood Hazards of Blood Transfusion
Stored RBCs • Increased deformity • Decreased 2,3, DPG • Metabolic acidosis • decreased oxygen carrying capacity • Increased red cell death with increased age of blood (~30% dead) • No improvement in oxygen utilization at the tissue level Hazards of Blood Transfusion
Distribution of Transfused Units by Age of Blood – CRIT Study 60% of Blood transfused is > 20 days old Percentage of Patients 0 - 10 10 - 20 20 - 30 30 - 40 > 40 Oldest Age of Blood in Days In Trauma Subset, 68% of blood is > 20 days old Hazards of Blood Transfusion
Guidelines for Blood Transfusion in Anemia • Anemia is common • No evidence that blood tx for treatment of anemia improves outcome • Critically ill patients can tolerate Hb levels as low as 7 mg/dL • Blood should be transfused for physiologic indications Hazards of Blood Transfusion
How to reduce the hazards? • RBCs should be administered as single units for most operative and inpatient indications (transfuse and reassess strategy) except for ongoing blood loss with hemodynamic instability. 1PRBC 1.3 gm/dl • Tx decisions are clinical judgments that should be based on the overall clinical assessment of the individual patient. Transfusion decisions should not be based on laboratory parameters alone. • Routine premedication is notadvised unless the patient has a history of previous transfusion reactions. Premedication has not been shown to reduce the risk of transfusion reactions. Hazards of Blood Transfusion
WHAT BEFORE ANY TRANSFUSION: • W- whether required?, when? • H- how much? • A- actual component required? • T- time duration and technique of transfusion? Hazards of Blood Transfusion
W- WHETHER REQUIRED? Indications: • Anemia- 60% • Surgery- 42% • Acute hemorrhage- 26% • Pregnancy- 16%. Seventy-four per cent of adult transfusions were inappropriate. Indian Study by Tim Bray et al Hazards of Blood Transfusion
W- WHAT TO TRANSFUSE? • Use Packed red cells to correct volume & oxygenation. • Uncontrolled bleeding and laboratory evidence of coagulopathy –Add fresh frozen plasma. • Bleeding continues :Consider Platelets after investigations. Hazards of Blood Transfusion
THRESHOLD FOR RED CELL TRANSFUSION: HISTORICAL FACTS • MAYO CLINIC in 1900 proposed a target value of 8-10 g/dL. • CURRENT PRACTICE (NIH Consensus) is 7g/dL in the absence of disease • 8-10g/dL in the presence of disease (cardiovascular disease/risk factors/elderly). • Rate of fall of Hb is more important than the actual Hb value • Healthy individuals tolerate Hb levels as low as 5g/dL Hazards of Blood Transfusion
FFP • More than 1 blood volume replaced • Prothrombin time prolonged with INR >1.5 and/or • Continued blood loss Dose: 15 ml/kg or 1 Litre (4 packs) for adult of 60 kg Hazards of Blood Transfusion
Platelets • Platelet count below 50 × 109/l (<50,000/ cmm), in the presence of bleeding. • Increased risk of hemorrhage in coagulopathy- <= 10000/mm3. • Vaginal deliveries or operative procedures ordinarily associated with insignificant blood loss may be undertaken in patients with platelet counts < 50,000/mm3. • Drop in Platelet below this level necessitates transfusion with platelet concentrates. Dose: 4-6 platelet concentrates or one unit of single donor (apheresis) platelets. Hazards of Blood Transfusion
Cryoprecipitate • If the fibrinogen is particularly low(<1g/l) or <100mg/dl. • Factor VIII deficiency • Early use of FFP may avoid the need for cryoprecipitate • Give 10 units initially and repeat based on fibrinogen estimation Note: Cryoprecipitate is not available from all blood centres. 5 units of FFP (1000-1250 ml) contains, typically, the same quantity of fibrinogen as 10 units of cryoprecipitate (approximately 150-250 ml) Dose: one unit/ 5 kg body weight or 10 units in the adult. Hazards of Blood Transfusion
Jehovah’s Witnesses and Associates - World Population • 1985 - 7,792,109 • 1995 - 13,147,201 • 2000 - 14,872,086 • 2007 - 16,675,113 Hazards of Blood Transfusion
What is Acceptable Risk? Hazards of Blood Transfusion
Thank you! Hazards of Blood Transfusion