Download
1 / 1
10 likes | 96 Views
Telephone Based Car e Management for Alcohol Misuse and Dependence. F. Zanjan i 2 , J.T. R oss 1,2 , C.Beswick 1 , V. Kamath 1 , M. Patterson 1 , I.R. Katz 1,2 , J. Seppelt 1 , V. Kane 1 , D.W. Oslin 1,2,3.

E N D
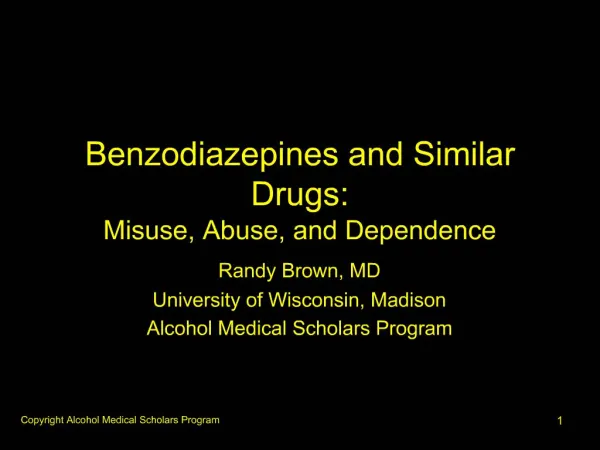
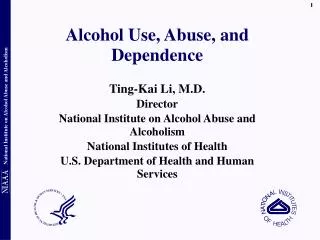
Telephone Based Care Management for Alcohol Misuse and Dependence F. Zanjani2, J.T. Ross1,2, C.Beswick1, V. Kamath1, M. Patterson1, I.R. Katz1,2, J. Seppelt1, V. Kane1, D.W. Oslin1,2,3 1. Mental Illness Research, Educational, and Clinical Center (MIRECC) at the Philadelphia VA Medical Center; 2. Section of Geriatric Psychiatry, University of Pennsylvania, Philadelphia, PA; 3. Center for the Study of Addictions, University of Pennsylvania, Philadelphia, PA; Abstract Methods Results – cont. Results – cont. • Screening is conducted by primary care staff using the AUDIT-C. For all patients who screen positively, the clinical reminder allows a direct referral to the BHL at the time of completing the screen. • Conducting the BHL Assessment: Health Technicians receive and register patient information from the consult in to the BHL database. Several attempts are made for each patient. If unsuccessful by phone, a letter is sent to the patient’s home address. All results, including those unable to contact, are documented to the PCP. (Table 1) • Assessments Conducted:. • Blessed Orientation-Memory-Concentration Test • International Neuropsychiatric Interview (MINI) for mania, psychosis, panic disorder, generalized anxiety disorder, PTSD, and alcohol abuse • PHQ-9 for depression • 5 item Paykel scale for suicide ideation • Current Anti-depressant Medication • Past and Current Use of Illicit Substances • Medical Outcomes Study (SF-12) • 4 item Patient Satisfaction scale • Assessment Outcomes: The computer algorithm scores all assessments and assigns patients into appropriate categories at completion of BHL assessment (Ongoing monitoring by PCP, appt in MH/SA clinic, or specialty care). Both the provider and the patients are sent a report of the outcomes of the assessment. • Care Management for those with appointments: Twenty patients given appointments with the mental health clinic were consented to be assisted with attending the appointment. Care Management consisted of three contacts with the patient throughout their treatment. Three telephone contacts were made, and involved obtaining the patient’s general goals, identifying substance abuse patterns, assessment of patient’s attitudes and obtaining a verbal agreement to attend the appointment. • Medical Record Abstraction and chart reviews: Medical Record Abstraction and chart reviews: Data from the clinical reminder for alcohol misuse screening (Audit-C) was retrieved from the electronic medical records. Chart reviews were conducted on those patients who required an appointment to be made for specialty MH/SA care. The chart reviews examined if the patients attended the appointments that the BHL staff made. • Data Analysis: Analysis was conducted on the Audit-C data, data from the BHL assessments, and data from chart reviews for the time period of July-October 2004. • Statistics: Descriptive Statistics (means, standard deviations, and frequencies), t-tests, Chi Square tests, and logistic regressions were used to examine outcomes. Analysis was conducted on the Audit-C data, data from the BHL assessments, and data from chart reviews for the time period of July-October 2004. Table 1.Characteristics of patients interviewed by the BHL All patients are categorized into one of 4 categories of severity based on the completed interview. Differences between severity groups are presented in Table 2. Objectives: The purpose of this project was to assess the utility and feasibility of a telephone based systematic clinical assessment service, the Behavioral Health Laboratory (BHL), in the context of primary care for patients with alcohol misuse. The BHL is a service that provides Primary Care Providers (PCPs) with a summary of mental health and substance abuse (MH/SA) symptoms and provides treatment recommendations, including triage to specialty MH/SA services. Methods: Results from AUDIT C screening of primary care patients were extracted during a period of 4 months. Descriptive results of the 94 BHL evaluations conducted during this time were available as well as information about treatment engagement. Results: Results demonstrate both the severity of problems but also the type of provider are important determinants of referral to the BHL. Referral for further assessment is low with an overall rate of 13% for those screening positive. This compares to approximately 60% referral rate for depression. However, the BHL was successful in assessing 78.9% of those referred and comorbidity was quite common among all referrals. While rates of engagement in care are low Telephone Care Management showed promise in engaging patients in treatment. Conclusions: The BHL offers a practical, low cost method of assessment, monitoring, and treatment planning for patients, identified in primary care, with MH/SA needs. Referral patterns for alcohol use appear very different than for depression suggesting significantly greater barriers to accessing alcohol care than depression care. Telephone monitoring and brief interventions appear effective in engaging patients in care. Conclusions Figure 2.Rate of Referral as a function of AUDIT- C Score Introduction • The BHL offers a practical and face-valid method of providing assessment and monitoring of mental health and substance abuse problems within primary care. • The BHL also offers the possibility of ongoing monitoring of symptoms for patients with specific MH needs. • In a cost effective manner, The BHL can overcome some of the problems in delivering quality mental health care, such as the already heavy demand on clinician time, availability of clinicians to conduct brief but frequent follow-up assessments, and the demand on patients for attending frequent follow-up visits. The BHL allows for rapid and systematic assessment of patients and can be an important tool for improving the management of depression and other mental health problems common in primary care. Results Routine screening for alcohol misuse in primary care settings is an important mechanism for reducing morbidity and mortality. Alcohol misuse includes a spectrum that ranges from risky drinking to alcohol dependence and has a well-demonstrated association with disability, increased health care utilization, and mortality. Since the prevalence of alcohol misuse is significantly higher among patients visiting a primary care practitioner than among the general population, primary care clinicians have the opportunity to play a key role in detecting alcohol misuse and in initiating prevention or treatment efforts. However, approximately half of primary care physicians rely only on clinical impressions to identify misuse. Therefore, many patients with alcohol misuse go unrecognized. Past research has shown that brief interventions within a primary care setting are effective in treating alcohol misuse, leading to sustained reductions in alcohol use, health care utilization, and alcohol related problems. The Behavioral Health Laboratory was developed as a clinical service to assist with providing comprehensive assessments for patients either by their clinician, or identified during routine care as potentially in need of mental health care. The BHL conducts all tests by telephone when ordered by the Primary care providers and sends test results back to PCPs together with guidelines for their interpretation and recommendations to assist in clinical decision-making. The purpose of this service was to implement a cost effective model that would substantially increase the feasibility of providing further evaluations and triage to the majority of patients referred to this service. Screening and Clinical Referral: Using a logistic regression model, we explored the likelihood of referring patients who screened positive for alcohol misuse to the BHL for the variables of total score and if the clinician was an MD or not. For every one point increase in total Audit-C score, the clinicians were 1.36 times more likely to refer to the BHL (p<.001) (Figure 1). If the clinician was an MD, the clinician was 3.62 times more likely to refer to the BHL than if the clinician were not an MD (p<.001) (Figure 2). Figure 1.Screening and Clinical Referral by provider type.* Selected References Clinical Referral: Based on the telephone assessment, 56.4% of those referred required additional evaluation in the MH/SA clinic. Of the 58 patients, 5 refused an appointment. Of the 53 patients given an appointment, 52.8 % attended a visit in the clinic within 3 months. • U.S. Preventive Services Task Force (USPSTF). Screening and Behavioral Counseling Interventions in Primary Care to Reduce Alcohol Misuse. Available at: http://www.ahrq.gov/clinic/3rduspstf/alcohol/alcomisrs.htm. • NIAAA. Screening for Alcohol Problems-An Update 2002. • American Society of Addiction Medicine. Screening for Addiction in Primary Care Settings 2001. • Wilk AI JN, Havighurst TC. Meta-analysis of randomized control trials addressing brief interventions in heavy alcohol drinkers. J Gen Intern Med. 1997;12:274-283. • Moyer A, Finney JW, Swearingen CE, Vergun P. Brief interventions for alcohol problems: a meta-analytic review of controlled investigations in treatment-seeking and non-treatment-seeking populations. Addiction. Mar 2002;97(3):279-292. • Fleming M, Barry K, Manwell L, Johnson K, London R. Brief physician advice for problem alcohol drinkers: A randomized controlled trial in community-based primary care practices. Journal of the American Medical Association. 1997;277:1039 - 1045. Referral Management: Of the 20 patients enrolled in Care Management, 70% (n=14) engaged in outpatient care, 45% (n=9) attended two appointments, and 40% (n=8) attended three or more appointments. TDMII: Of those with who were eligible for a VA sponsored research study, Telephone Disease Management for At-Risk Drinking (n=8), 4 agreed to participation. This study is based on brief alcohol intervention literature and aims at reducing alcohol use or engaging patients in more formal treatment. *Values represent means (standard deviations) for continuous measures and percentages for categorical measures. BHL Assessment Within the timeframe between August 1, 2004-October 31, 2004, of the 906 patients who screened positive for alcohol misuse,118 patients were referred to the BHL. Of those 118 patients that were referred to the BHL, 78.9% completed the assessment, 5.9% refused and 14.4% were unable to contact. For the 118 referred to the BHL, the mean age was 54.19 (12.46), 12.7% were over 65, and 98.3% were male (Table 1). Costs of Assessments: Considering cost of staffing, laboratory maintenance, administrative expenses, and program level expenses, the total cost of the BHL per assessment is approximately $45.26 per initial assessment and $25.13 per follow-up assessments.