Download
1 / 43
440 likes | 588 Views
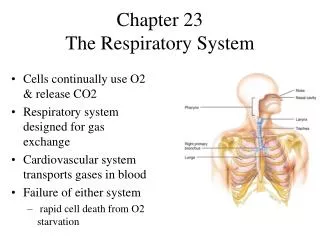
The afferent visual system is broadly designed to achieve 2 fundamental goals : to detect the presence of objects within the environment. to provide a high level of spatial resolution for those objects that command our attention.

E N D
The afferent visual system is broadly designed to achieve 2 fundamental goals: • to detect the presence of objects within the environment. • to provide a high level of spatial resolution for those objects that command our attention
The entire retina outside of the fovea is devoted essentially to the detection of objects. Only the fovea, which occupies a tiny fraction of the total retinal area, provides the fine-quality images that allow us to read or perform highly precise visuomotor tasks.
Any imprecision in maintaining alignment of the fovea on the moving target degrades the appearance of the image. • The need to maintain high-quality vision despite any “relative movement” is addressed by multiple ocular motor systems .
SYSTEMS THAT CONTROL EYE MOVEMENT Pursuit system OKN system Saccadic system vergence system vestibular These are each controlled by different anatomic pathways.
pursuit system • To track relatively slow moving targets (no faster than 30° per sec). • Can do it through vestibulo -ocular reflexes (VOR), which produce eye movements in a direction opposite to that of head movements. • The VOR, however, attenuate fairly quickly (ie, within seconds) during a persistent period of relative motion.
Smooth pursuit • Slow conjugate eye movement • Voluntary or involuntary • To keep image of a moving object at fovea • Mediated by parieto-occipito-temporal-mesencephalic pathway • Ipsilateral control
optokinetic nystagmus (OKN) system • Provides The capability of following objects over a sustained period of motion. • (OKN) system uses smooth pursuit to track a moving object but then introduces a saccade in the opposite direction when the maximal amplitude of the pursuit movement is reached or when the speed of the moving object exceeds the maximal velocity of the pursuit system
OKN • Slow conjugate eye movement • Involuntary • To keep retinal images fixed during prolonged head / body rotation • Unknown pathway • Response to acceleration • Fades with sustained constant speed of rotation
saccadic system • Relatively fast moving targets cannot be tracked but can be followed by the use of relatively fast, back-to-back eye movements generated by the saccadic system. • saccades, are “ballistic” movements—ones that cannot be altered once initiated
saccade • Fast conjugate eye movement • Voluntary • To bring object images to the fovea • Mediated by fronto-mesencephalic / superior colliculus pathways • Contralateral control
Persistent foveation is controlled by microsaccadic refixation movements .
vestibular • Depends on vestibular motion receptors in the semicircular canals in each ear and the labyrinthine-pontine pathway • Stimulation of horizontal canal results in horizontal nystagmus • Stimulation of posterior canal results in vertical nystagmus • Stimulation of anterior canal results in rotational nystagmus • Contralateral control
vestibular • Produce a slow conjugate eye movement • Involuntary • To keep retinal images fixed during brief head / body rotation.
Fixation:the ability to maintain attention on an object Convergence/divergence: the ability for the eyes to turn in and turn out so they are aimed at the same place in space. Saccades:the ability of the eyes to uniformly track, stop at an indicated position, resume movement and return to a preset position.
Stereopsis: the ability of eyes and brain to interpret the presented information as a three dimensional image. • Rotations and versions:testing the eye muscles tracking (following) a moving object. • Accommodation test: tests the focusing/de-focusing opticalsystem in the eye. • Cover Test:to determine if the eyes are properly aligned for a given distance.
Binocular Single Vision • the state of simultaneous vision, which is achieved by the coordinated use of both eyes, so that separate and slightly dissimilar images arising in each eye are appreciated as a single image by the process of fusion.
Motor Fusion • It is the ability to align the eyes in such a manner that sensory fusion can be maintained. The stimulus for these fusional eye movements is retinal disparity outside panum’s area .
Oculomotor paresisresults in a limitation of saccades in specific directions relative to the head (rightward, leftward, upward and downward). One possible solution is to adapt the head position relative to the display so that the entire display remains accessible with eye movements.
Ocular nystagmusis a constant oscillation of the eye which results in an inability to maintain a stable fixation. • One possible solution is to find the head position which minimizes the amplitude of the oscillation.
Strabismusis another condition where only one eye is fixating while the other eye is deviating from that direction. • Phoriais a condition where deviation appears only after some delay, for example as a result of fatigue.
Examination of the eyeball Observe the following points A) Position – normally the two eyeball are symmetrically placed in the orbit in such a way that a line joining the center point of superior and inferior orbital margins just touches the cornea Dr Sanjay Shrivastava 18 November 2014 21
Examination of the eyeball b) Visual axis of eyeball • Normally the visual axis of the eyeball is simultaneously directed at same object which is maintained in all the directions of gaze. • Deviation is the visual axis of one eye is called squint. Dr Sanjay Shrivastava 18 November 2014 22
Examination of the eyeball c) Movement of eye ball The movement are tested uniocular (duction) as well as binocularly (versions) in all the 9 diagnostic positions of gaze. Uniocular – Adduction, abduction, depression, elevation, depression and elevation in adduction and abduction
Visual acuity • Inspection • Evaluation of ocular alignment • Version test Others to aid Dx of supranuclear disorders • Convergence test • Saccades’ and pursuits’ movements • Doll’s eye movement • OKN test • Caloric responses
Ocular motility examination Look at ( inspection) head posture: 1) Face turn- towards side of weakness e.g. 6th CN palsy ,Duane’s 2) Head tilt- e.g. away from side of 6th CN palsy. 3) Chin up/down e.g. bilateral 6th CN palsy
(Inspection) • Ptosis - 3rd CN palsy • Primary position – manifest strabismus • Corneal reflexes – asymmetry indicates deviation. • Pupils-anisocoria
Evaluation of ocular alignment • Corneal reflection tests -Hirshberg’s test -krimsk’s test -Bruckner’s test • Cover tests -Cover/uncover -Alternate cover - prism cover test
HIRSHPERG’S TEST • Detect gross heterotopias • Based on purkinje sanson image no.1 • Look at symmetry of light reflex • Normal reflex….just nasal to center of pupil • Abnormal reflex….each 1 mm of deviation =7 degrees = 30 PD
COVER TESTS • Based on fixation ability • Normal fixation behavior….CSM • Cover/uncover …detect manifest deviation • Alternate cover ….detect total deviation ( manifest + latent)– dissociation test • To measure angle of deviation….prism cover test
Check versions ( both eyes) and ductions (one eye) in all 9 positions of gaze -ask patient to follow target ( pen-torch) -perform cover test in each position -ask patient to report any diplopia during test look for any abnormality; under/overaction, paresis/restriction .
Examination of EOM Binocular Ocular Movements 3 3 4 5 4 5 1 2 1 2 6 7 8 6 7 8 Right side Left side 1 = Dextroversion; 2 = Levoversion; 3 = Elevation; 4 = Dextroelevation ; 5= Levoelevation; 6= Dextrodepression; 7= Depression; 8 = Levodepression
If there is any diplopia ……… indicates deviation • Uncrossed diplopia = eso –deviation • Crossed diplopia = exo – deviation • Hypertropic eye will see the lower image
Ocular misalignments may be comitant or incomitant. • Incomitant misalignments indicate an innervational problem or a mechanical restriction. • Ductions (ie, movement of a single eye with the other eye covered) may be better than versions in patients with innervational problems, with no difference between ductions and versions noted in patients with mechanical restrictions. • Forced ductions are restricted with mechanical disease and normal with paralytic disease, unless the paralysis has caused chronic contracture of the muscle.
In patients with CN III palsy, the presence or absence of afferent pupillary involvement must be documented. Pupil-involving lesions may indicate an underlying posterior communicating artery aneurysm, and neuroimaging studies are required.
If a vertical deviation is noted, head tilts are performed…( parks-bielschewsky 3-step test) • To identify a single underacting muscle in vertical / torsional deviation. • Particularly useful in SO palsy • 3 steps • Identify hypertropic eye • Identify gaze where disparity is greatest • Identify head tilt side where disparity is greatest
Examine horizontal/vertical saccades • ask patient to look rapidly between widely separated targets result: ---normal / slow hypo/ hypermetric • Useful in detecting internuclear ophthalmoplegia • Smooth pursuit is tested by having the patient slowly follow a moving target 1m a way.
Separating saccades from smooth pursuit may be clinically important. Smooth pursuit may be irregular in brainstem- cerebellar disease, and catch-up saccades may be required. • In Parinaud syndrome, upgaze saccades may be affected more than upward smooth pursuit early on in the disease. • In patients with small pontine strokes involving purely the paramedian pontine reticular formation (PPRF), saccades may be affected and smooth pursuit relatively preserved. This is because the fibers of the latter eye movement system do not synapse in the PPRF.
Examine convergence assess to both accommodative and non- accommodative target normal / reduced …….Hold a target in front of patient and progressively bring it nearer , whilst observing for convergence of the two eyes
Examine Doll’s eye movement Normal / absent • When a horizontal gaze palsy is suspected • Hold the head of the patient and rotate it from side to side …………if the eyes deviate fully it indicates intact pontine reflexes ……… supranuclear lesion
Examine OKN -horizontal / vertical • slowly rotate an OKN drum in horizontal and vertical direction result : Normal / absent /convergence retraction( vertical gaze palsy) • Useful in cases of parinaud’s syndrome
Caloric response • Caloric testing is dependent on endolymph convection currents. • Normal response • Warm water in the right ear produces a right-beating nystagmus • coldwater in the right ear produces a left-beating nystagmus