Download
1 / 30
300 likes | 774 Views
D2-40 immunohistochemistry in the differential diagnosis of seminoma and embryonal carcinoma: a comparative immunohistochemical study with KIT (CD117) and CD30. Modern Pathology (2007) 20, 320–325 Sean K Lau, Lawrence M Weiss and Peiguo G Chu

E N D
D2-40immunohistochemistry in thedifferential diagnosis of seminoma andembryonal carcinoma: a comparativeimmunohistochemical study with KIT(CD117) and CD30 Modern Pathology (2007) 20, 320–325 Sean K Lau, Lawrence M Weiss and Peiguo G Chu Department of Pathology, City of Hope National Medical Center, Duarte, CA, USA Intern 鄭詩燕
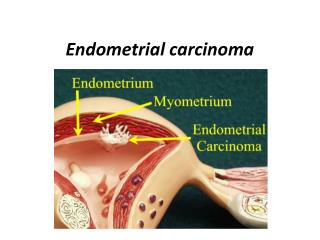
Testis: Germ Cell Tumors • Seminoma • Nonseminomatous Embryonal carcinoma Yolk sac (endodermal sinus)tumor Choriocarcinoma Teratoma
Seminoma • Age: 15-35y/o • 50% of germ cell tumor • Painless swelling • Dysgerminoma in ovary
Seminoma • Bulky masses, sometimes 10 times> the normal testis. • Homogeneous, gray-white, lobulated cut surface, usually devoid of hemorrhage or necrosis • Mostly the entire testis is replaced. • Occasionally, extension to the epididymis, spermatic cord, or scrotal sac
Seminoma • Seminoma Cell: large and round to polyhedral and has a distinct cell membrane • A clear or watery-appearing cytoplasm • A large, central nucleus with one or two prominent nucleoli • The cytoplasm contains varying amounts of glycogen. • AFP(-) or HCG(-), placental alkaline phosphatase(+), 15%HCG(+)
Embryonal carcinoma • 20- to 30-year age group. • Grow faster than seminoma • Painful • More aggressive than seminomas
Embryonal carcinoma • Size: smaller than seminoma • Usually does not replace the entire testis. • The mass is often variegated, poorly demarcated at the margins • Punctuated by foci of hemorrhage or necrosis • Extension through the tunica albuginea into the epididymis or cord is not infrequent.
Embryonal carcinoma • The cells: alveolar or tubular patterns, sometimes with papillary convolutions • Undifferentiated cells, epithelial appearance • Hyperchromatic nuclei with prominent nucleoli. • Indistinct cell border, variation in cell and nuclear size and shape, mitotic figures • HCG(+), AFP (+)
Introduction • Some seminomas : increased nuclear pleomorphism, cell crowding, and lack a lymphocytic infiltrate -> confusion with embryonal carcinoma. • Limited biopsy specimen or poor tissue fixation.
Introduction Immunohistochemistry • CD 30: Embryonal carcinoma(+), Seminoma(-), Mixed germ cell tumors(+/-) • KIT(CD117): Seminoma(+), Embryonal carcinoma(-) Mixed germ cell tumors(+/-)
Introduction • D2-40 Monoclonal antibody reacts with an oncofetal membrane antigen (M2A) which present in testis fetal germ cells Intratubular germ cell neoplasia, seminoma(+), Embryonal carcinoma(-)
Materials and methods • 40 cases of testicular germ cell tumor • Age 18-41, mean age: 30 • Pure germ cell tumor (26 cases) 19 seminomas, 3 embryonal carcinomas,3 teratomas, 1 yolk sac tumor • Mixed germ cell tumors(14 cases) 7 seminomas, 11 embryonal carcinomas, 10 teratomas, 2 yolk sac tumors, and 1 choriocarcinoma.
Materials and methods • Immunohistochemical staining: D2-40, KIT, CD30 • Xylene (deparaffinized) and ethanol (dehydrated) • Slide heating in EDTA buffer(pH8) in pressure cooker • Automated immunostainer -> antibody detection, counterstained with hematoxylin and coverslipped.
Result 26 14
Result • D2-40 antibody Seminoma -- strong membranous Embryonic carcinoma -- weak, focal, distributed along the apical or luminal surfaces of the cells.
Discussion • D2-40 recognizes M2A antigen which present in fetal germ cells, lymphatic endothelium, and mesothelial cells. • M2A antigen expression in all seminomas and seminomatous components of mixed germ cell tumors
Discussion • Present study: -- D2-40 in pure or mixed seminoma: 100% (26/26), (mixed) embryonal carcinoma 29% (4/14) -- Seminoma: diffuse membrane staining -- Embryonal carcinomas: focal and confined to the apical or luminal surfaces. • Marks et al study -- D2-40 in seminomas 98%, embryonal carcinomas 69%.
Discussion • Distinction between seminoma and embryonal carcinoma can be madeon a morphologic basis using conventional histologicmethods. • Studies addressing theimpact of central histopathologic review of previouslydiagnosed testicular tumors have demonstratedmajor discrepancy rates of 4–11%
Discussion • Immunohistochemical markers: keratins, KIT, and CD30. • Antikeratin antibodies -- Embryonal carcinoma : keratin intermediate filaments -- Seminomas lacked • Recent study -- Keratin positive in seminomas 4 to 45% • KIT and CD30: more effective immunohistochemical markers
Discussion • Previous study KIT expression in seminoma: 100% • Present study KIT expression in seminoma: 92% none in embryonal carcinomas or non seminomatous germ cell tumors
Discussion • CD30: as a sensitive as well as a specific maker for embryonal carcinoma (93%) • Focal CD30 expression has been described in a subset of seminomas • Leroy et al CD30 in combination with KIT -- seminoma: KIT(-), CD30(+) impossible -- embryonal carcinoma: KIT(+), CD30(-) impossible
Discussion • Present study Sensitivity: D2-40 > KIT in seminomas Specific: D2-40 < KIT in seminomas (4/11 embryonal carcinomas +) • D2-40 in seminomas: diffuse and membranous • D2-40 in embryonal carcinomas: focal and limited to the apical or luminal surface of the cells.
Summary • KIT and CD30: a useful markers that allows for seminoma to be distinguished from embryonal carcinoma. • Although a highly sensitive marker of seminomas, focal D2-40 immunoreactivity can be seen in a subset of embryonal carcinomas, thus limiting the practical value of this marker for discriminating between these particular malignancies.