Download
1 / 28
280 likes | 421 Views
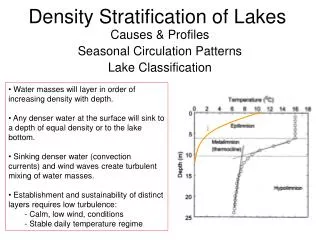
Risk Stratification & Intervention. Follow Up Care for High Risk Patients Mary Beth Byrnes, MSN, RN. CARE MANAGEMENT PROCESS. Identify High Risk. Planned Care at Every Visit Risk Assessment Chart Alerts Registry Reports Notification from Hospital Admission & Discharge Notification

E N D
Risk Stratification & Intervention Follow Up Care for High Risk Patients Mary Beth Byrnes, MSN, RN
Identify High Risk • Planned Care at Every Visit • Risk Assessment • Chart Alerts • Registry Reports • Notification from Hospital Admission & Discharge Notification • Self-Reporting
Risk Stratification • Age • Co-existing Health Conditions • Number of Medications • Functional Deficits • Non-adherence to treatment plan • Self-Care & Knowledge Deficits • Socio-Economic Issues • Support System • Utilization
Depression Risk Factors • Age • Co-Morbidities • Number of Medications • Significant Loss - Spouse, other significant family member, pet • Family Care Giver (Spouse or other generational dependent) • Social Isolation/Absence of Social Support • Fatigue/Sleep Disturbance • Chronic Pain • Functional Disability • Current Alcohol/Substance Abuse Disorder • Psychosocial Causes • Cognitive Distortions • Chronic Stress • Poor Self-Health Rating
Risk Factors for Falls • Age (>80 Years of Age) • History of Falls • Gait Dysfunction • Balance Dysfunction • Use of Assistive Devices • Visual Deficit • Medications (Hypotensive, CNS Suppressants) • Arthritis/Chronic Pain • Diarrhea/Urinary Frequency • Impaired ADL’s • Depression • Cognitive Impairment
Cumulative Risk • 0 – 1 Risk Factors – Seniors have a 27% chance of a fall each year • >4 Risk Factors – Seniors chance of a fall increases to 78% each year Tinetti: 1998
Interventions • Evidence Based Guidelines • Functional Deficits • Knowledge Deficits • Socio-economic Issues • Barriers to Achieving Goals • Support System
High Risk Follow Up • Follow Up Date & Method Agreed Upon • Task List with Scheduled Reminder • Identify Goals Met – Unmet • Identify Barriers to Unmet Goals • Revise Plan • Set Next Follow Up
85 Year Old Male • Hypertension on 1 medication • Active and Working until 02/2011 • Fell on ice injuring ribs (1st Fall) • Hospitalized for abdominal pain with subsequent cholecystectomy • SNF • Severe Depression – Short Time in Mental Health System • 02/2011 to 01/2012 • Fell 3 more times – Out of State/County • Fracture Hip (01/2012) • Fell at Home 5 weeks after discharge (5th Fall) • Readmitted surgical repair wound dehiscence • Did not know family members until 01/2012
Goals & Barriers • Self-Management Goals • Increase Physical Activity • Increase Self-Care Activities • Barriers • Difficulty Dealing with Functional Loss • Inability to Recognize Depression • Inability to Recognize Need for PT
Interventions • Inpatient & Outpatient PT/OT • Home Care • Evaluation of Home Environment – Fall Prevention • Medication & Psychiatric Counseling • Respite Care – 1 Week • Ongoing Outreach – Patient & Wife • Encourage Participating in ADL’s and Movement • Transitional Care Nurse