Download
1 / 37
420 likes | 602 Views
Mental Health and HIV. Objectives. List 3 crisis points for HIV infected persons List 4 most commonly diagnosed clinical disorders in HIV+ population Understand/explain when screenings should occur Explain how mental health issues affect HIV+ population. Mental Health and HIV.

E N D
Objectives • List 3 crisis points for HIV infected persons • List 4 most commonly diagnosed clinical disorders in HIV+ population • Understand/explain when screenings should occur • Explain how mental health issues affect HIV+ population
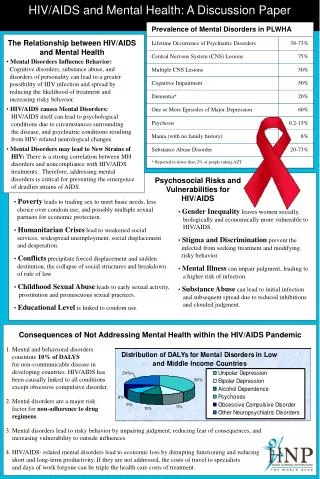
Mental Health and HIV • People with HIV are much more likely to experience mental health problems than individuals in the general population • Nearly 50% of participants screened positive for one or more of four psychiatric disorders • The groups most likely to screen positive for mental illness include: • Individuals under age 35 • African Americans • People who lived alone or with a non-romantic partner • Unemployed/ disabled • Those with more HIV-related symptoms • Those who reported using illicit drugs other than marijuana From: “Mental Health and Substance Abuse Issues Among People with HIV: Lessons from HCSUS”
Mental Health and HIV • Though HIV primarily affects men in the US, a high proportion of women who were participants in the study tested positive for some form of mental illness • Respondents tended to be younger, who had more advanced disease, and who needed income assistance • Most individuals with HIV who have mental health problems receive the treatment they need, but earlier detection and intervention would likely offset the increase medical costs they often incur • 70% of respondents was estimated to need mental health care (including SA treatment) • 70% of these individuals did receive care From: “Mental Health and Substance Abuse Issues Among People with HIV: Lessons from HCSUS”
Mental Health and HIV • HIV+ individuals with mental health issues are less likely to receive HAART, and those that do are less likely to comply • Primary factors influencing lack of adherence to HAART for individuals with mental health issues: • Time and effort it takes to get the medications • Challenges of integrating complex treatment regimens into one’s lifestyle From: “Mental Health and Substance Abuse Issues Among People with HIV: Lessons from HCSUS”
Mental Health and HIV • How do mental health issues affect HIV risk? • How do mental health issues affect the perception of risk?
Mental Health and HIV HIV Risk HIV Risk Perception
Screening for Mental Health • Why screen for mental health? • Mental health issues are a risk factor for noncompliance with medical treatment • Mental health issues are correlated to non-adherence • Mental health issues are a predictor of clinical progression of HIV disease, independent of non-adherence behavior* • Specifically, studies show a correlation between depression and clinical progression of disease* • Correlation between mental health issues and risky behaviors • Including substance use, injection drug use, unprotected sex • Who do you screen for mental health issues? • Everybody! • How often should you screen for mental health issues? • Formal screening at baseline and at required recertification times (every 6 months for MCM, every 12 months for N-MCM) • Informal screening during all regular contacts for individuals with current mental health issues or recent history of mental health issues • When co-morbid issues arise • Non-compliance with medical treatment • Indicators of substance abuse/dependence *Mental Health, Substance Abuse and HIV/AIDS – Relationship and Response; Nick Curry.
Screening for Mental Health • Crisis points for HIV infected persons • Learning of HIV-positive status • Disclosure of HIV status to family and friends • Introduction of medication • Occurrence of any physical illness • Recognition of new symptoms/progression of disease (e.g., major decrease in CD4 cells, increase in viral load) • Necessity of hospitalization (particularly the first hospitalization) • Death of a significant other • Diagnosis of AIDS • A return to a higher level of functioning (e.g., re-entry into job market/school, giving up entitlements) • Major life changes (e.g., childbirth, pregnancy, loss of job, end of relationship, relocation) • Necessity of making end-of-life and permanency planning decisions New York State Department of Health. Depression and mania in patients with HIV/AIDS. New York (NY): New York State Department of Health; 2008 Jun.
DSM-IV • The DSM-IV organizes each psychiatric diagnosis into five levels (axes) relating to different aspects of disorder or disability: • Axis I: Clinical disorders, including major mental disorders, as well as developmental and learning disorders • Axis II: Underlying pervasive or personality conditions, as well as mental retardation • Axis III: Acute medical conditions and physical disorders. • Axis IV: Psychosocial and environmental factors contributing to the disorder • Axis V: Global Assessment of Functioning or Children’s Global Assessment Scale for children under the age of 18. (on a scale from 100 to 0)
DSM-IV • Axis I – Clinical Disorders • Common diagnoses among HIV+ population: • Depression • Anxiety disorders (including PTSD) • Bipolar disorder • Schizophrenia
Major Depressive Episode • Five (or more) of the following symptoms have been present during the same 2-week period and represent a change from previous functioning; at least one of the symptoms is either (1) depressed mood or (2) loss of interest or pleasure. • Depressed mood most of the day, nearly every day, as indicated by either subjective report or observation made by others • Markedly diminished interest or pleasure in all, or almost all, activities most of the day, nearly every day • Significant weight loss when not dieting or weight gain, or decrease or increase in appetite nearly every day. • Insomnia or hypersomnia nearly every day • Psychomotor agitation or retardation nearly every day • Fatigue or loss of energy nearly every day • Feelings of worthlessness or excessive or inappropriate guilt nearly every day • Diminished ability to think or concentrate, or indecisiveness, nearly every day • Recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide.
Major Depressive Episode • Patients co-infected with hepatitis C virus (HCV), patients receiving treatment with interferon, and patients with disfiguring side effects of antiretroviral (ARV) therapy, particularly body fat changes, are more prone to develop depressive symptoms. *New York State Department of Health. Depression and mania in patients with HIV/AIDS. New York (NY): New York State Department of Health; 2008 Jun.
Major Depressive Episode • How does this present with our clients? What do we need to listen for – what are the red flags?
Anxiety Disorders • A subjective experience of distress with accompanying disturbances of sleep, concentration, social and/or occupational functioning are common symptoms in many of the anxiety disorders. • Generalized Anxiety Disorder • Social Anxiety Disorder • Obsessive-Compulsive Disorder • Post-Traumatic Stress Disorder • Phobias and Panic Disorder • While there are similarities, these disorders often differ in presentation, course and treatment.
Anxiety Disorders • How does this present with our clients? What do we need to listen for – what are the red flags?
Bipolar Disorder • Bipolar I • Required one or more manic or mixed episode • May include hypomanic and depressive episodes • Though not required, depressive episodes are common • Bipolar II (most common) • Episodes of both hypomania and depressive episodes • Cyclothymia • Numerous hypomanic episodes intermingled with depressive episodes that don’t meet the full criteria for a major depressive episode • Does not interfere with functioning
Hypomanic Episode • A distinct period of persistently elevated, expansive, or irritable mood, lasting throughout at least 4 days, that is clearly different from the usual non depressed mood. • During the period of mood disturbance, three (or more) of the following symptoms have persisted (four if the mood is only irritable) and have been present to a significant degree: • inflated self-esteem or grandiosity • decreased need for sleep • more talkative than usual or pressure to keep talking • flight of ideas or subjective experience that thoughts are racing • distractibility • increase in goal-directed activity or psychomotor agitation • excessive involvement in pleasurable activities that have a high potential for painful consequences
Manic or Mixed Episode • Manic Episode • Same criteria as Hypomanic, except it lasts for at least a week • Mixed Episode • The criteria are met both for a Manic Episode and for a Major Depressive Episode nearly every day during at least a 1-week period
Manic Episode • How does this present with our clients? What do we need to listen for – what are the red flags?
Schizophrenia • Two (or more) of the following, each present for a significant portion of time during a 1-month period (or less if successfully treated): • Delusions • Hallucinations • Disorganized speech (e.g., frequent derailment or incoherence) • Grossly disorganized or catatonic behavior • Negative symptoms, i.e., affective flattening, alogia, or avolition
Schizophrenia • Social/occupational dysfunction: For a significant portion of the time since the onset of the disturbance, one or more major areas of functioning, such as work, interpersonal relations, or self-care, are markedly below the level achieved before the onset. • Duration: Continuous signs of the disturbance persist for at least 6 months. • This 6-month period must include at least 1 month of symptoms (or less if successfully treated) that meet active-phase symptoms
Schizophrenia • How does this present with our clients? What do we need to listen for – what are the red flags?
DSM-IV • Axis II – Personality Disorders • Experience and behavior that deviates markedly from the expectations of the individual's culture. This pattern is manifested in two (or more) of the following areas: • cognition (perception and interpretation of self, others and events) • affect (the range, intensity, lability, and appropriateness of emotional response) • interpersonal functioning • impulse control • The enduring pattern is inflexible and pervasive across a broad range of personal and social situations. • The enduring pattern leads to clinically significant distress or impairment in social, occupational, or other important areas of functioning. • The pattern is stable and of long duration and its onset can be traced back at least to adolescence or early adulthood.
Personality Disorders • Cluster A (odd or eccentric disorders) • Paranoid personality disorder: characterized by irrational suspicions and mistrust of others • Schizoid personality disorder: lack of interest in social relationships, seeing no point in sharing time with others • Schizotypal personality disorder: also avoids social relationships, though out of a fear of people
Personality Disorders • Cluster B (dramatic, emotional, or erratic disorders) • Antisocial personality disorder: "pervasive disregard for the law and the rights of others." • Borderline personality disorder: extreme "black and white" thinking, instability in relationships, self-image, identity and behavior • Histrionic personality disorder: "pervasive attention-seeking behavior including inappropriate sexual seductiveness and shallow or exaggerated emotions • Narcissistic personality disorder: "a pervasive pattern of grandiosity, need for admiration, and a lack of empathy"
Personality Disorders • Cluster C (anxious or fearful disorders) • Avoidant personality disorder: social inhibition, feelings of inadequacy, extreme sensitivity to negative evaluation and avoidance of social interaction • Dependent personality disorder: pervasive psychological dependence on other people. • Obsessive-compulsive personality disorder (not the same as Obsessive-compulsive disorder): characterized by rigid conformity to rules, moral codes, and excessive orderliness
DSM-IV • Axis III - Includes brain injuries and other medical/physical disorders which may aggravate existing diseases or present symptoms similar to other disorders • Axis IV - Includes issues with support group, housing problems, income problems, education problems, economic problems, problems accessing health care, legal problems
DSM-IV • Axis V – Global Assessment of Functioning 91-100 Superior functioning in a wide range of activities, life's problems never seem to get out of hand, is sought out by others because of his or her many qualities. No symptoms. 61-70 Some mild symptoms OR some difficulty in social, occupational, or school functioning, but generally functioning pretty well, has some meaningful interpersonal relationships. 21-30 Behavior is considerably influenced by delusions or hallucinations OR serious impairment in communications or judgment OR inability to function in all areas. 1-10 Persistent danger of severely hurting self or others OR persistent inability to maintain minimum personal hygiene OR serious suicidal act with clear expectation of death.
DSM-IV • Multiaxial Evaluation
Working with Clients with Mental Health issues Barriers to beginning/maintaining substance abuse treatment • Clients • Weak provider network/inaccessible resources (multiple agencies) • Overly pushy/confrontational providers • Other problems with therapeutic relationship • Providers • Client willingness/motivation • Financial resources • Weak provider network • Transportation Capacity Building Project: Serving the Mental Health and Substance Abuse Needs of HIV Infected Persons in Texas; 2010. Texas DSHS.
Working with Clients with Mental Health issues Primary factors that played a role in clients’ decision to begin/maintain substance abuse treatment • Providers • Case manager involvement • Good rapport with staff/providers • Accessible services • Client’s feelings about themselves • Transportation • Clients • Rapport with provider • Effective therapeutic techniques • Internal drive • Willingness Capacity Building Project: Serving the Mental Health and Substance Abuse Needs of HIV Infected Persons in Texas; 2010. Texas DSHS.
Maintaining Clients with Mental Illness in Care • Assess clients’ psychosocial status regularly—housing, employment and/or social security disability benefits, health insurance, family and partner contacts, stability of relationships, including domestic violence screening • Ask follow-up questions of clients regarding mental health and treatment progress as a routine part of sessions • Make referrals to mental health care if the client is not receiving mental health care • Monitor adherence to recommended mental health treatment, including psychotropic medications, appointments with mental health providers, and attendance in support groups • Maintain follow-up phone contact with clients’ mental health treatment programs, including notifying programs of medication changes (w/ release of information) • Monitor clients’ potential barriers to adherence to ARV therapy when applicable Mental Illness in Patients With HIV/AIDS: HIV Clinical Guidelines for the Primary Care Practitioner. New York State Department of Health AIDS Institute: www.hivguidelines.org
Case Study #1 • Ricardo is a 41 year old man who has been in case management for two years. Recently during an appointment, Ricardo indicated some depressive symptoms, and screened positive on a mental illness screen. Ricardo stated he did not want any doctor putting him on any medications, but reluctantly agreed to schedule an appointment w/ an LCSW who see clients at your clinic. Ricardo is back in to see you two weeks following his scheduled appointment w/ the LCSW and you know that he did not keep his appointment.
Case Study #1 • Education – client may not understand difference between therapist/LCSW and psychiatrist • Assess stage of change/important/confidence – where is client really at, what does he really want. May have pushed too far ahead of where client was • The client keeps his appointment with you – don’t assume he missed his appointment because he didn’t want to go. Talk to client about reasons why he missed.
Case Study #2 • Macy is a 40 year old woman who is a new case management client who was referred to case management by the infectious disease doctor at your clinic. Prior to meeting Macy, the ID doctor tells you that Macy has schizophrenia and he’s been told that she’s being treated, but he’s unsure exactly how. The ID doctor wants to start Macy on medications, but is hesitant to do so yet until he feels that she is more stable. You meet w/ Macy and a guardian, who the state recently appointed. Macy is primarily homeless, but does occasionally stay at a boarding house. The guardian tells you that the woman (a local restaurant owner whom Macy has asked to be her payee for her SSDI check) who had been giving Macy her anti-psychotic had only been giving her ½ the prescribed dosage, because she could only get Macy to come by once a day and she figured that was better than nothing. Macy is very reluctant to speak to you and refuses to answer many of your questions and tells you that you’re ‘being a nosy bitch’ and that it’s ‘none of your business’.
Case Study #2 • How much autonomy does client have with a state guardian in the picture? • Very important to coordinate care between client’s doctors (psych and ID) so there both aware of the care that’s being provided • What is the psychiatrist actually prescribing? Is there a regiment that could fit with her lifestyle better? • Client trusts her payee – bringing the payee in on the care team (with client permission) may be beneficial in building trust with client, and having somebody else in the client’s life to reinforce the correct messages • Client still answers some questions – find out what she will talk about, and start with that (even if it’s unrelated to client health). • May be able to use supportive services/community referrals (food, bus tokens, etc.) to engage client in medical care initially • Have to get client stable before looking at HIV treatment • Constant education – need to assess client’s ability to understand/literacy/health literacy and start establishing a foundation of knowledge • Talk to client – don’t “talk” to client through guardian or payee