Download
1 / 25
250 likes | 549 Views
OPERATION IRAQI FREEDOM Army on the Ground in OIF; Combat Stress Care Initiatives. COL Jim Stokes, MC. USA Combat/Operational Stress Control Program Officer, USAMEDCOM San Antonio, TX james.w.stokes@us.army.mil 210-221-8235/DSN 471-. DISCLAIMER.

E N D
OPERATION IRAQI FREEDOM Army on the Ground in OIF; Combat Stress Care Initiatives COL Jim Stokes, MC. USA Combat/Operational Stress Control Program Officer, USAMEDCOM San Antonio, TX james.w.stokes@us.army.mil 210-221-8235/DSN 471-
DISCLAIMER While data from the Mental Health Advisory Team (MHAT) will be presented, the opinions expressed are those of COL Jim Stokes, and do not necessarily represent those of the MHAT, the Army Medical Department, the Department of the Army or the Department of Defense.
AGENDA Mental Health Advisory Team (MHAT) Overview of observations Soldier Well-Being Survey findings Methodology and survey sample Stressors reported Unmet needs of Soldiers in OIF for COSC/BH support Army Combat/Operational Stress Control (COSC) Where is Army COSC in OIF (operations/organization)? Stats on rRturn to Duty of soldiers evaluate/treated The Challenge of Accountability Relevance to BH Care of Disaster Responders
MHAT Requested by CJTF7 and CFLCC Command. Chartered by The Army Surgeon General. (“The Mysterious Twelve”) All 5 BH/COSC disciplines plus Chaplain, DCSPER’s Suicide Prevention Proponent (Inf.), Ist SGT and SFC (MH & CSC backgrounds), and 2 Researchers from WRAIR REPORT:www.armymedicine.army.mil
MHAT(continued) In Kuwait/Iraq from late Aug to Oct ‘03 • Observed, analyzed COSC and BH system • Scientific survey (1st ever) in a combat stability and support operation • Soldier Well-being Scale (756 Soldiers, many in daily danger, combat), followed by Focus Groups • Structured Individual Interviews of Leaders, Chaplains, Primary Care providers, BH providers
OVERVIEW OF FINDINGS The MHAT was impressed (awed) with the professionalism, dedication and resilience under severe stress of the many Soldiers we saw and the few we talked with in the study. Most griped, but remarkable mission focus. The COSC support system was working well under the strain. It worked mostly with the relatively small number of soldiers in severe distress (for many reasons) and kept most of those treated “forward” on duty. Travel between CSC teams and units at remote camps was risky & time/resource expensive.
SOLDIER WELL-BEING SURVEYFINDINGS in September ‘04 STRESSORS REPORTED CombatOperational (One or More Times) (High/Very HighConcern) Saw human dead67%? Redeployment date ?87% Small arms fire 63%Long deployment71% Attack/ambush61%Separated from family57% Knew someone 59% No privacy or personal 55% seriously injured space or killed
MORALE & COHESION in Sep ‘03 • Soldiers were surveyed about personal and unit morale: • 52%of Soldiers reportedlow/very low morale • 72%of Soldiers reportedlow/very low unit morale • Non-combat deployment stressors were significantly correlated with low personal and unit morale • Uncertain re-deployment date p < .05 • Longer deployment length (days)
SOLDIER WELL-BEING SURVEYFINDINGS in Sep ‘03 (cont’d) • 77%of Soldiers surveyed reported none to lowstress, emotional, alcohol or family problems Moderate =16 % Severe = 7 % • 83%of Soldiers did not meet screeningcriteria for Behavioral Health functional impairment. • 17.2%did reported symptoms of the one or more of the following, with social and/or occupational impairment. Anxiety Depression Traumatic Stress 7.3% 6.9% 15.2%
SOLDIER WELL-BEING SURVEYFINDINGS in Sep ‘03 (cont’d) • Combat stressors and uncertain redeployment date correlate significantly with symptoms of anxiety, depression and/or traumatic stress StressorSignificance Level • Being attacked or ambushedp < .001 • Duration in a hostile area • Engaging in a firefightp < .05 • Uncertain re-deployment date
SOLDIER WELL-BEING SURVEYFINDINGS in Sep ‘03 (cont’d) • Of the Soldiers who screened positive for Anxiety, Depressions and Traumatic Stress, only 27% reported receivinghelp at any time from a BH professional, general medical doctors or chaplain. • Of the 15% of all Soldiers who reported interest in receiving help, only 32% received some form of help.
SOLDIER WELL-BEING SURVEYFINDINGS in September ‘04 • Soldiers want help, but perceive barriers to care • Soldiers who screened positive for anxiety, depression or traumatic stress were twice as likely to perceive barriers. • Screened Screened Perceived Practical Barriers PositiveNegative Difficulty getting time off work 43% 16% Difficulty getting to BH location 26% 10% Don’t know where to get help 24% 11% BH services not available 24% 10% Difficult to get an appointment 19% 8%
SOLDIER WELL-BEING SURVEYFINDINGS in September ‘04 • Perceived stigma was also cited by Soldiers as an important concern when considering seeking care for BH problems Perceived Barriers answered YES . Might be seen as weak 59% Unit leaders might treat them differently 58% Unit would have less confidence in them 49% Their leaders would blame them for the problem 48%
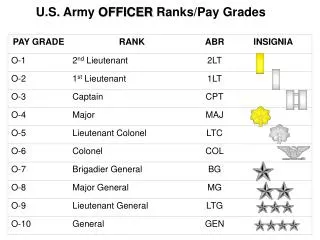
WHERE WAS ARMY COSC IN OIF? • NOT NEW: Built onWWI, WWII, Korea, Vietnam, Gulf War,contingency ops, OEF. • NOT“Teams of counselors roaming around the battlefield….” Rather are… • A BH officer + tech embedded in most brigades • A psychiatrist + NCOIC in each Division • CSC Detachments that augment each Division • CSC Company teams dispersed over Corps, and with teams in separate brigades & ACRs,
COSC ORGANIZATION • Divisions have Psychiatrist, Psychologist, Social Worker • CSC Units have those, plus Psychiatric Nurses, Occupational Therapists • Detachment has 5-8 four-person teams • Company has up to 14 such teams. • All are usually based at Medical Companies; to provide mobile outreach to supported units • BH PROVIDERS : TROOPS IN IRAQ = 1:830
INSUFFICIENT TRAINING IN COSC “PREVENTIVE” DOCTRINE • Over 50% of BH providers in theater (including hospital staff) reported they didn’t know COSC doctrine or didn/t support it. • 50% said they had not had adequate COSC training and over 50% wanted more intense COSC training. • Issue: How to reconcile the “disease” model of diagnosis and treatment with the COSC preventive model of “normal reactions in abnormal situations”?
INHIBITIONS TO ACTIVE OUTREACH • Tendency to stay with the familiar clinic model. Outpatient caseload builds up. • Lack of authorized vehicle; few radios. • Difficulty of arranging convoy • Risk, even following Force Protection rules • Introverted personality • Stretched thin SOME TEAMS did MAGNIFICENT OUTREACH!
RETURN TO DUTY PERCENTAGES OF COMBAT/OPERATIONAL STRESS REACTIONS & MENTAL DISORDERS • 95% by Division, CSC teams forward . . (doesn’t include Helped In Place) • 85%(+/-) from CSC Restoration • 69% from Cbt Spt Hosp Psych Svc + . . CSC in Baghdad Green Zone • 11% from CSH in Kuwait • 3% from Landstuhl, Germany
NEED CLARIFICATION OF COSC FUNCTIONS All disciplines do all functions within each individual’s scope of practice. • Consultation/Education Includes Unit Needs Assessment • Critical Event/ Transition Managment • COSC Triage (PIES / BICEPS) • Stabilization • Soldier Restoration (1-3 day holding) • Soldier Reconditioning (4-7 day holding, plus) Also BH Treatment which keeps SM on duty
MY OBSERVATIONS • The MHAT documented a significant, hidden, unmet need for BH support to troops who have not become “stress casualties”, and probably won’t. • Forward-deployed Brigade/CSC teams work. Properly trained Behavioral Health personnel have essential skills they can share with others in combat scenarios. • Where active outreach is done despite the effort and risk, it is very well received and effective in sustaining unit functioning. • The Antidote to Stigma is Presence • Proactive BH/COSC Prevention in support of Command is necessary to keep service members functioning effectively and reduce risk of long- term negative outcomes.
COSC DOCTRINE’S PRIMARY INTENTION IS PREVENTION MHAT found clearer guidance is needed. • UNIVERSAL – for everyone in area • SELECTED – for those at high risk • INDICATED – for those with early . signs and symptoms • TREATMENT – for those with DSM . diagnosis, to keep on duty
THE CHALLENGE OF ACCOUNTABILITYIt’s inherently hard to prove preventive work’s value. • Workload accounting of preventive inter- vention (surveillance and mitigation) is essential to: • Document what has been done for which units and individuals • Plan and coordinate further activities • Report to higher headquarters BH consultant • Reallocate and plan for resources • Monitor trends and test hypothesis • Determine short and long term outcomes • Do cost/benefits analysis.
COMBAT/OPERATIONAL STRESS CONTROL- WORKLOAD ACTIVITY RECORDS/REPORTS SYSTEM (COSC-WARS) • Prototype formats for documenting preventive contacts, individual contacts, and summary reports. • Tested “manually” by some units, and the summary report became the standard for CSC units to send weekly to Med Brigade HQ. • Now is approaching pilot test with all formats automated, collatable, etc.
RELEVANCE TO DISASTER RESPONSE • Is there a similar unmet BH need in the Disaster Response community? • Physical time/distance barriers to getting BH advice and coaching? • Similar perceived stigma? • Similar potential for active outreach to enlighten leaders and service members (from the front lines to the support workers and families) • Remember, Army COSC will be part of Military Support to Civil Authority in major disasters.
Save Questions to end. COL Jim Stokes, MC. USA COSC Program Officer, USAMEDCOM, San Antonio, TX james.w.stokes@us.army.mil 210-221-8235/DSN 471- MHAT REPORT www.armymedicine.army.mil