Download
1 / 11

E N D
CIMT Constraint-Induced Movement Therapy Please note: This view-only presentation is based on one therapist’s opinion and experience ONLY! It assumes that clinicians will rely on their own critical appraisal of the evidence, and their own knowledge and expertise when prescribing this intervention to clients with a stroke-affected upper limb.
CIMT: Objectives In this view-only presentation, we’ll look to answer the following questions: • What is it? • Does it work? • Who should it be prescribed to? • What dose did we use? • What do I recommend?
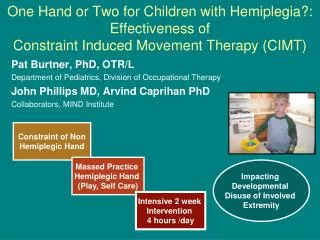
CIMT: What is it? CIMT = Constraint-Induced Movement Therapy • It’s used to overcome learned non-use • It’s a sub-type of repetitive, task specific practice (RTP) • It’s a combination of RTP and a constraint! NB: I’m going to use the term ‘client’ to refer to a client or patient Isobel’s notes: What’s learned non-use? Good question! It’s a problem specific to the upper limb (UL) and one that I refer to as the “hopping problem”. You see, with the lower limb, following stroke it becomes fortunate that it’s more difficult to hop than it is to walk because it means that learned non-use is not as much of a problem. But…. with the UL, (as anyone knows who’s had a broken arm or a new baby,) people can quite quickly learn to do things reasonably successfully using just one UL (hopping). And, once you’ve learnt to do things this way, if you have a stroke-affected UL, it can become difficult to revert back to using both Uls. This is what’s meant by the term “learned non-use” – and yes, it’s more of an UL issue. This is a really important point! There’s NO evidence that simply putting a mitt on a stroke survivor’s less affected arm and hand (upper limb) for lots of hours a day for a few weeks will ensure better recovery of the more affected upper limb!
CIMT: What’s RTP? CIMT = RTP plus a constraint component • RTP = lots of repetitive task-specific practice • We used the Canadian Occupational Performance Measure to identify 5 tasks that were most important to the client. This meant that the RTP element was client-centred or relevant • We accepted all tasks except driving a vehicle. If driving was in the top 5, we included task 6 • See examples of the logs used to ensure lots of repetitivepractice • These 5 tasks became the basis of the CIMT/RTP program. It’s my observation that most tasks have an UL component • Each task was listed onto an individual card. At the start of each RTP session, the cards were shuffled to make sure that the order the tasks were practiced in, was random Isobel’s notes: There are 5 things I was wanting to ensure; that RTP was random, repetitive, relevant to person and place, and reinforced. For more detail, I refer you to my publication: Hubbard et al (2009) Occupational Therapy International, 16 (3-4)
CIMT: What’s the Constraint? CIMT = RTP plus a constraint component • Constraint = thumbless mitt or sling. We used... • A thumbless mitt, but some therapists use a sock! • Therapist-made mitts in two sizes using calico, wadding and Velcro • Three pieces of fabric with lots of wadding sewed into the palm area between two layers • A Velcro attachment which fastened loosely at the wrist • The 5x5x5 dose for wearing the constraint: 5 consecutive hours a day, 5 days a week, for 5 weeks • We recommended that it not be worn when home alone and not when using the toilet • We found all clients were compliant with using the mitt Isobel’s notes: As a first-time CIMT prescriber, I was reluctant to use a sling because I worried that the client/patient might fall. And perhaps this worked because we recorded no adverse events, but who knows. The mitt meant that the user could still move the less affected UL to support or steady themselves – and it meant I was less worried as the prescribing therapist!!
CIMT: Does it work? Isobel’s personal opinion: CIMT is one of the most researched UL interventions to date! I don’t know of any other intervention that’s had to go through so much rigorous investigation, and yet, it’s still not prescribed by many therapists. I’m not sure why this is the case! We’ve been routinely applying interventions that have not been so rigorously studied, but for whatever reason, CIMT has had to sustain a more rigorous level of investigation than other interventions we routinely use!! And, even though it’s in most nationally-agreed clinical guidelines, we’re still cautious about prescribing it!! Were we this sceptical about Bobath, Motor-relearning or Functional Electrical Stimulation? Were they all as rigorously investigated? CIMT has sustained animal modelling studies, randomised controlled trials and systematic reviews. I can’t help but ask: What more proof do we need that its works in certain stroke survivors? From my ‘read’ of the evidence, CIMT is effective in: • Clients with 20º of active movement at the wrist and 10º in the finger/s and/or thumb • Chronic survivors (1,2) • Acute survivors: conflicting evidence (3,4) NB: CIMT is recommended as an UL intervention in the Australian nationally-agreed clinical guidelines (5) • Hakkennes S, Keating JL (2005). Constraint-induced movement therapy following stroke: a systematic review of randomised controlled trials. Australian Journal of Physiotherapy 51:221–231 • Smania et al (2012) Reduced-intensity modified CIMT vs conventional therapy……Neurorehabilitation & Neural Repair, 26(9), 1035-1045 • Dromerick et al (2009) Very early CIT during stroke rehabilitation (VECTORS): A single-center RCT. Neurology, 73(3), 195-201 • Page et al (2005) Modified CIT in acute stroke: a randomised controlled pilot study. Neurorehabilitation & Neural Repair, 19, 27-32 • National Stroke Foundation (2010) Clinical Guidelines for Stroke Management (p.87) http://strokefoundation.com.au/site/media/clinical_guidelines_stroke_managment_2010_interactive.pdf
CIMT: Which clients? CIMT should only be prescribed to those with: • Stroke: this can be within a few days (acute) or months or even years post event (chronic) • Some observable movement in the more affected UL. The benchmark = 20º/10º group • Those who are able to comply with the constraint and RTP components. • We successfully prescribed CIMT in clients who could accurately respond to a 2-step command
CIMT: Which clients? …cont We used CIMT successfully in the following cohort: • Community-dwelling adult survivors of a first ischemic stroke • Clients who were at least 3 months post stroke and were not living alone Please note, this is not to say that the above group are the ONLY or BEST group to prescribe CIMT to – the evidence indicates otherwise. But I’m just qualifying which group we used it in. I don’t want to misrepresent what we did, but I also don’t want to undermine the evidence or what’s recommended in the Australian nationally-agreed clinical guidelines.
CIMT: What dose did we use? The following is what worked for us: For 5 consecutive weeks…… • Face-to-face time = 1x3x5: 1 hour, 3 times a week. Usually with an Occupational Therapist and sometimes with a therapy assistant • RTP ≥ 2x5x5: at least 2 hours a day, 5 days a week. • Mitt wearing = 5x5x5: 5 consecutive hours a day, 5 consecutive days a week • Clients maintained a participation log - see sample copy • Therapist revised the participation log each week Isobel’s Notes: Perhaps this was too much; but it was within the parameters of what other studies had used in this cohort, successfully. We had no clients that pulled out, no adverse events and everyone was pleased with the outcome. It took me by surprise. I know, I shouldn’t have been surprised, because the evidence was telling me it would work in this group, but I was, nevertheless!! (Duh!!) The clients were surprised too - and all the more, because no one had prescribed it to them previously!! Miraculous? Well yes, to be honest, a little!!
CIMT: In my humble opinion… Constraint-induced Movement therapy should: • Be included in the standard care ‘tool kit’ for those with a stroke-affected 20/10 UL • Be considered as a clinically effective 20/10 UL intervention for those with learned non-use • NOT be “optional” for this group because it’s evidence-based and included in clinical guidelines • Always include an RTP and constraint component
CIMT Constraint-Induced Movement Therapy Please note: This view-only presentation is based on one therapist’s opinion and experience ONLY! It assumes that clinicians will rely on their own critical appraisal of the evidence, and their own knowledge and expertise when prescribing this intervention to clients with a stroke-affected upper limb.