Download
1 / 23
240 likes | 1.29k Views
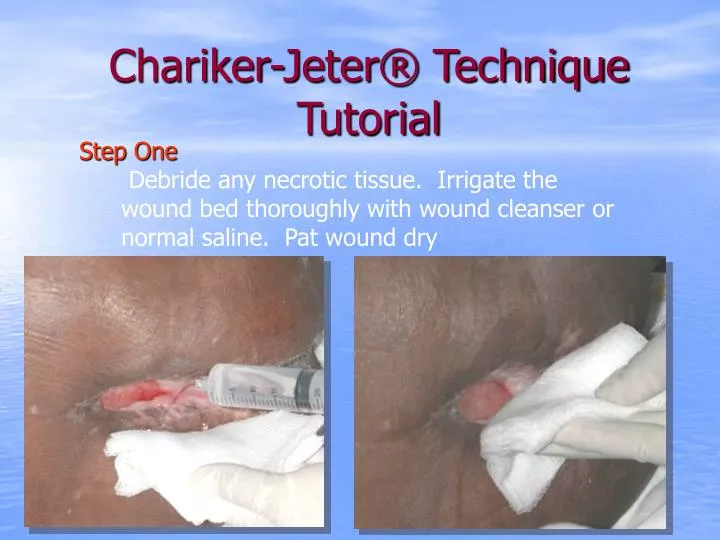
Chariker-Jeter® Technique Tutorial. Step One Debride any necrotic tissue. Irrigate the wound bed thoroughly with wound cleanser or normal saline. Pat wound dry. Step Two.

E N D
Chariker-Jeter® TechniqueTutorial Step One Debride any necrotic tissue. Irrigate the wound bed thoroughly with wound cleanser or normal saline. Pat wound dry
Step Two • Apply skin sealant to all skin that will be covered by transparent adhesive skin dressing. Allow skin to dry until sticky.
Step Three • Open the Aquaphor dressing, cut a single layer to the appropriate size and shape of the wound bed. • Lay the Aquaphor dressing across the wound bed.
Next • Shorten Jackson Pratt Catheter as necessary so that the flat drain is confined to the wound bed (recommend 1” shorter than wound bed). Place Catheter between saline moistened fluffed gauze (the catheter is never placed into a fistula tract or directly onto pink granulating tissue). Fill dead space with saline moistened fluffed gauze or roll gauze. Chariker, Jeter, 1989
Step Four • Place the Jackson-Pratt suction catheter/drain on top of the Aquaphor dressing. • The drain should not come into direct contact with the wound bed. • Shorten the drain as necessary so that the flat drain is confined to the wound bed. (The drain should never be placed in a fistula tract.)
Step Five • Open the 4x4 gauze pads. Saturate with normal saline. • Fluff into wound to completely cover the drain and fill the defect to skin level.
Step Six • Cover the entire packed wound with the transparent dressing carefully moving the tubing to either side of the wound. The dressing should allow for at least 1” of intact skin beyond the wound edges.
Step Six continuedSealing the Wound Dressing • Crimp or pinch the edges of the transparent film around the tubing to secure a proper seal. • You may use stoma-adhesive paste or a hydrocolloid to fill any gaps caused by a skin fold to ensure appropriate seal. • You may also reinforce this junction with pink waterproof tape or other adhesive tape.
Next Place the supplied tube clamp over the end of the drain tube and connect to canister, with connecting tube and supplied adapter.
Step Seven • Insure that overflow/bacteria filter is on pump. • Use Canister with Mechanical overflow lid device. • Fill with sterile water after estimating drainage to be collected. • Be sure that filter connection tubing is attached to the vacuum port on the canister as this will assure proper overflowshutoff protection !!!
Canister Fill If canister size does not match estimated drainage, simply fill canister with sterile water to achieve desired level i.e. pictured canister has a volume of 800cc if we expect the wound to drain 300cc between dressing / canister changes we put 500 cc of sterile water in the canister. Canister Volume – Estimated Drainage = Volume of Sterile water to add.
Step 8continued • Turn pump on and adjust to upper range of low setting, (60-80 mm Hg) observe the site. • The dressing should contract noticeably. If it does not you do not have a closed system and will need to find/patch the leak. • You may patch with a piece of transparent film. • Once an airtight seal is reached, adjust the pump to the prescribed negative pressure.
Monitoring the Patient • Insure that protocol is present for Closed Suction Wound Drainage. • Patients need to be monitored(i.e. don’t ignore patient for 3 days) Replace Chariker-Jeter dressing @ 48 hours initially and then every 2-3X per week as indicated.
Insure Good Outcomes • Make sure that a protocol is present for Closed Suction Wound Drainage. • Patients need to be monitored • Check pump for proper vacuum setting. • Document canister contents for type/color, odor and amount of exudate. • Check for air leak using procedure below. • Check dressing at shift change or every 8 hours by using clamp to occlude tubing. If dressing balloons and contracts when clamp is applied and released; leak is present and needs to be sealed. Also have patient, nurse or caregiver listen for any leaks.
Dressing Changes • Frequency and extent depend on the status of the patient, i.e. infection, excessive drainage… • Initial dressing change at 48hrs and then as long as no leakage is present, patient is comfortable and pump is effective at pulling fluid; recommended changing 2-3X/wk
Patients/Wounds Not Indicated • Malignancy • Nutritional Compromised- < 2.0 Albumin • Organs, blood vessels, major structures exposed • Untreated Osteomyelitis • Multi-system failure to thrive • Systemic steroids • Uncooperative or unsuitable candidates
Clinical Indications to D/C Wound Suction • Completion of successful course of treatment • Pain at wound site • Wound fluid has reduced to the point that there is a dry wound bed • Patient preference