Download
1 / 4
40 likes | 320 Views
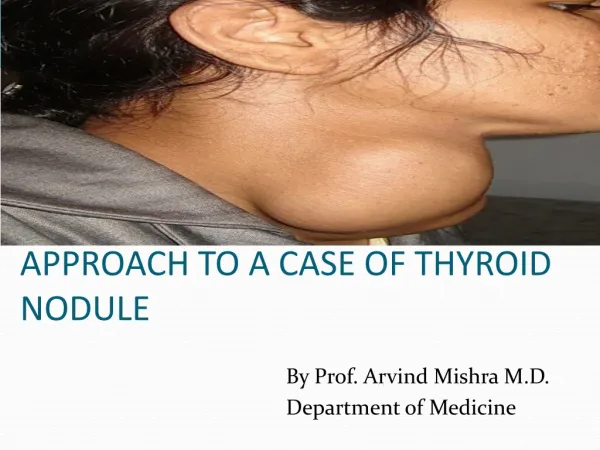
Thyroid Nodule. Kenny DeSart , M.D. Neck/Thyroid Nodule. Do they have increased risk? Extremes of age Rapid growth Family history History of radiation Check TSH Normal/elevated-proceed with FNA If low, get thyroid scan, if Hot nodule will need with ablation or resection.

E N D
Thyroid Nodule Kenny DeSart, M.D.
Neck/Thyroid Nodule • Do they have increased risk? • Extremes of age • Rapid growth • Family history • History of radiation • Check TSH • Normal/elevated-proceed with FNA • If low, get thyroid scan, if Hot nodule will need with ablation or resection
Fine-Needle Aspiration • Typically ultrasound guided • 75-90% Determinant • Benign-Malignant-Suspicious-Indeterminant-Inadequate • Benign-follow patient for changes • Suspicious-surgical resection (follicular/hurthle) • Indeterminant • Repeat FNA, Open biopsy, surgical resection • Papillary carcinoma • 80-90% thyroid cancer, most common and least aggressive • Psammoma bodies and Orphan Annie nuclei • Lobectomy if <1cm • Total thyroidectomy • >1cm, bilateral dz, positive margins, multicentricity, history of radiation • If extrathyroidal or clinically positive nodes, add MRND • 131-iodine if metastatic, residual local disease, positive nodes, capsular invasion • Follicular cells • 5-10% chance of malignancy (unable to differentiate b/t adenoma/hyperplasia/cancer) • Lobectomy and f/u pathology, may need completion thyroidectomy if carcinoma • Follicular carcinoma • Total thyroidectomy +/- MRND if nodal/extrathyroid tissue involvement • 131-iodine 6wks postop if tumor >1cm or extrathyroidal
Fine-Needle Aspiration • Medullary carcinoma • MEN IIa/IIb-screen for hyperparathyroidism/pheochromocytoma • Prophylactic thyroidectomy at age 2 in kids • Total thyroidectomy with central node dissection • MRND if clinically positive nodes • Hurthle cell carcinoma • FNA unable to differentiate b/t Hurthle cell adenoma • Total thyroidectomy + MRND for clinically positive nodes • Anaplastic thyroid cancer • Aggressive and lethal • Total thyroidectomy if resectable (rare), consider palliative chemo/XRT • Lymphoma • Metastatic disease • Cystic-drain fluid, send for cytology • Close follow-up, if it recurs may repeat aspiration, if it recurs again--perform lobectomy/thyroidectomy