Download
1 / 23
230 likes | 494 Views
Current Treatment Options in MDS. Dick Wells MD, DPhil, FRCPC Director, Crashley Myelodysplastic Syndrome Research Laboratory Odette Cancer Centre. Mr. Blue Low Hb, WBC, platelets >90% chance of developing leukaemia within 2 years Life expectancy about 18 months. Ms. Green Anaemia only

E N D
Current Treatment Options in MDS Dick Wells MD, DPhil, FRCPC Director, Crashley Myelodysplastic Syndrome Research Laboratory Odette Cancer Centre
Mr. Blue Low Hb, WBC, platelets >90% chance of developing leukaemia within 2 years Life expectancy about 18 months Ms. Green Anaemia only ~10% chance of developing leukaemia ever Life expectancy more than 10 years Tale of Two Patients They both have MDS, but do they both have the same disease?
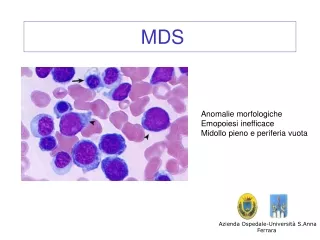
MDS is at least two diseases • Some patients (“high risk”) have a severe disease that rapidly evolves into acute leukaemia • Others (“low risk”) have a chronic disease that makes them anaemic
Low Risk MDS To alleviate anaemia and to minimize the harm caused by transfusion High Risk MDS To prevent the development of leukaemia and to extend lifespan Different situations, different goals
Treatment Options for High Risk MDS-prevent leukaemia, extend lifespan • Supportive/palliative care • Allogeneic bone marrow transplantation • Donor not always available • High risk, high relapse rate
Is that all there is?Other options for high risk MDS Hypomethylating drugs • Vidaza (Pharmion) • Dacogen (MGI Pharma) What they do: “Rehabilitate” bone marrow cells in MDS by changing their pattern of gene expression
Hypomethylating drugs:Clinical trials • Vidaza and Dacogen beat supportive care • Major responses in 20-25% • Responders remained or became transfusion independent and symptoms improved • Duration of response <1year • Delayed time to AML progression or death • Trend toward improved survival
Dacogen x 18 cycles 2u PRBC/wk
Upside Improve counts Delay leukaemia May improve survival Improve quality of life Downside NOT AVAILABLE! Expensive Not everyone responds Temporary responses Best duration of treatment unknown Forever? Hypomethylating drugs for MDS
Treatment Options for Low Risk MDS-alleviate anaemia, reduce transfusion harm • Transfusion • 90% of patients • Iron chelation • To remove excess iron due to transfusion • “Growth factors” • To boost red blood cell production • Immune suppression • To protect developing blood cells
Epo and Red Blood Cells • Red blood cells carry oxygen • If not enough oxygen gets to the kidney, epo is released • Epo tells the bone marrow to make more red blood cells Giving extra epo can help boost haemoglobin in MDS
Upside Easy Not toxic Can get transfusion independence Downside Expensive Needles! Not everyone responds Temporary responses No effect on platelets or WBC Growth factors for MDS
Immune Suppression • The theory: • In MDS, as in aplastic anaemia, the immune system attacks the bone marrow. Drugs that block the immune system may help. • The evidence: • About 50% of MDS patients respond to this sort of treatment
Upside Durable responses Can improve all blood counts Downside Expensive Very toxic (especially ATG) Not everyone responds Immune suppression in MDS
Is that all there is?Other options for low risk MDS Revlimid • “Cousin” of thalidomide • Many biological activities • Early studies: amazingly active in patients with MDS and chromosome 5 abnormalities
Deletion 5q [del(5q)]A problem with the long arm… • Most frequent chromosomal deletion in MDS patients • 10-20% (+/- other abnormalities) • 5-6% as sole abnormality • Better-than-average prognosis • Low risk of leukaemia
MDS-003 trialRevlimid in 5q- MDS • 67% of patients achieved transfusion independence • 90% of patients who achieved a transfusion benefit did so by completion of 3 months of therapy • Durable responses (>2 y) 67% Transfusion Independence(99/148 patients) List et al., N Eng J Med, 355, 1456, 2006
Start Lenalidomide Haemoglobin Last Transfusion Platelets
Start Lenalidomide Haemoglobin Neutrophils G-CSF 300 mcg BIW
“Doc, I’m a new man!” Last Transfusion Haemoglobin Start Lenalidomide
Upside Amazingly active in 5q- MDS Oral, once daily Pretty easy to take Currently available on SAP; Health Canada approval around the end of 2007 Downside Lowers WBC and platelet counts (initially) Expensive! Restricted to low risk 5q- MDS Revlimid in MDS
If 5q-, revlimid If epo<500, try growth factors Immune suppressive therapy (ATG and/or cyclosporine) If feasible, BMT Supportive/palliative care …or clinical trial … or hypomethylating drugs Summary:Algorithms for MDS