Download
1 / 97
970 likes | 1.6k Views
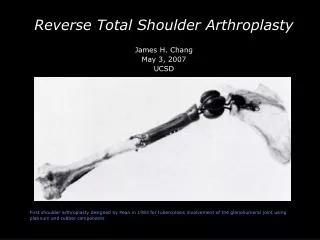
Proximal Humerus Fractures ORIF & Arthroplasty. Reza Omid, M.D. Assistant Professor Department of Orthopaedic Surgery Keck School of Medicine of USC. Introduction. 5-7% of all fractures 80% treated nonoperatively (Neer) Bimodal incidence

E N D
Proximal Humerus Fractures ORIF & Arthroplasty Reza Omid, M.D. Assistant Professor Department of Orthopaedic Surgery Keck School of Medicine of USC
Introduction • 5-7% of all fractures • 80% treated nonoperatively (Neer) • Bimodal incidence • Bone quality- important factor in obtaining secure fixation
Etiology Elderly • fall onto outstretched hand • direct blow- fall • bone fragility- a/w distal radius fractures Young • high energy • seizures, electrical injury
OITE Facts • How many with neurologic injury? • 21-36% • recent study- 45%- fx or dislocation on EMG • Which nerves? • Axillary, suprascapular, radial, musculocut. • How many with persistent motor loss? • 8%
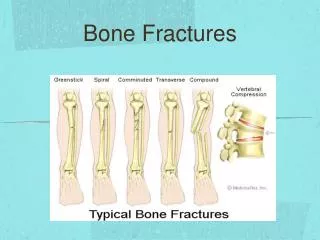
Neer’s Classification Codman’s Description
Classification Neer’s classification Sidor, Zuckerman, JBJS 1993 Gerber, JBJS, 1993 • poor inter and intra observer reliability • best results among trained shoulder surgeons • suggested CT scans would increase reliability
Proximal Humeral Anatomy Understanding Fracture Patterns • 4 bony fragments • Lesser Tub • Greater Tub • Head • Shaft Neer, JBJS ‘70
Proximal Humerus Assesment Neer Classification • 1 cm displaced • 45 deg angulated • Excessive rotation
Proximal Humerus Fractures Fracture Patterns • Stable • Fx not controlled by muscle • Unstable • Fx controlled by attached muscle
Proximal Humerus Fracture Fracture Anatomy • Greater Tub – posterior, proximal • Lesser Tub – medial, inferior • Head – remaining tub or fx energy • Shaft – medial, superior
X-Rays AP view scapular plane (Grashey) AP view of shoulder
X-Rays Axillary Lateral Scapular Y
Proximal Humerus Fracture Radiographic Analysis • Normal Appearance • Axillary: lesser tub, greater tub not seen
Proximal Humerus Fracture Radiographic Analysis • Normal Appearance • AP: external rotation shows greater tub • AP: internal rotation, greater tub not seen
Proximal Humerus Fracture Fracture Anatomy
Consideration for Surgery Bone Quality Comorbidities Functional demand Vascularity???
Gerber JBJSAm 1990: 1486-94 Vascularity • anterior humeral circumflex • Anterolateral branch Of AHC (arcuate artery) Along lateral aspect of groove
Brooks JBJSBr 1993: 132-136 • Vascularized through interosseous anastomoses • Between metaphyseal vessels (via posterior humeral circumflex) and the arcuate artery after ligation of the anterior circumflex humeral.
Coudane JSES 2000: 548 • Arteriography done on 20 patients after proximal humerus fractures. • 80% had disruption of AHC artery • 15% had disruption of PHC artery • Since AVN is rare (bw 1-34%) after fx it suggests the PHC artery may be dominant supply
Hettrich JBJSAm 2010: 943-8 • MRI cadavers • posterior humeral circumflex • supplied 64% of head (superior, lateral and inferior).
Hertel Criteria Hertel et al JSES 2004:13:427 • Medial calcar segment <8mm • Medial hinge is disrupted (>2mm displacement of the diaphysis) • Comminution of the medial metaphysis • Anatomic neck fracture
Bastian JSES 2008: 2-8 • Follow-up study by Hertel showed that initial predictors of humeral head ischemia doesn’t predict development of AVN. • 80% of patients with “ischemic heads” did NOT collapse • Fixation is worth considering even if signs of ischemia are present
Nonoperative Treatment Immobilize initially Passive ROM 2-3 weeks • supine FE • supine ER • pendulums AROM at 6 weeks or when consolidated 77% good to excellent results-Zuckerman 1995
Optimal Treatment • UNKOWN???? • JSES 2011: 1118-1124 (RCT ORIF vs Non-op) • JSES 2011: 747-55 (RCT ORIF vs Non-op • JSES 2011: 1025-1033 (RCT Hemi vs Non-op) • JOT 2011 (RCT ORIF vs Non-op)
Percutaneous PinningSurgical Technique • Retrograde Pins • Start Anterior • Diverge Pins • Antegrade Pins • Supplemental • GT to Medial Shaft
Percutaneous PinningReduction Maneuver • Surgical neck • flexion, adduction, traction • anterior pressure • Greater tuberosity • engage and move anteriorly/inferiorly
Pin Placement Slight medial placement of head to shaft Allows placement of one pin centrally Wide spread of pins for stability *Remember normal humeral head retroversion for pin placement Pin entry is just above the deltoid insertion Pins Three 2.5mm terminally threaded pins 2 lateral pins 1 anterior pin 1-2 pins from GT to medial shaft Percutaneous Pinning Jaberg H. JBJS. 74A. 1992. 508-15.
Cadaveric Study Lateral pins 3mm from Ant branch Ax Penetration of head articular cartilage Anterior pins 2mm from biceps tendon 11mm from cephalic v. Proximal tuberosity pins 6-7mm from ax n. & posterior circumflex artery Structures At Risk Rowles DJ, McGrory JE. “Percutaneous Pinning of the Proximal Part of the Humerus. JBJS. 83A(11)2001.1695-99.
Starting point of proximal lateral pin At or distal to a point 2x the distance from the superior aspect of the humeral head to the inferior margin of the head Greater tuberosity pins Engage medial cortex >2cm from the inferior most aspect of the humeral head Recommendations Rowles DJ, McGrory JE. “Percutaneous Pinning of the Proximal Part of the Humerus. JBJS. 83A(11)2001.1695-99.
Greater Tuberosity Fractures Displacement • Superior • Impingement • Posterior • Block to ER
Greater Tuberosity Fractures Displacement? • 5mm maybe problematic (McLaughlin et al.) • 3mm maybe problematic in the athlete or heavy laborer (Park et al.) • Concern for RTC tears in minimally displaced fxs Positioning critical • *Exposure • Approach: Superior, Posterior, Anterior Reduction • Head height 6-8mm superior to GT • Posterior displacement more tolerated than superior displacement
Greater Tuberosity Fractures • Surgical Approach • Superior • Deltopectoral • Fixation Options • Sutures • Screws • Plate • Interval Closure
Three-Part Fractures Surgical Neck + Greater Tuberosity Lesser Tuberosity
Three-Part Fractures Fixation Options • Percutaneous Pins • Interfragmentary Suture/Wire • Plate/Screws • IM Nail • Blade Plate • Hemiarthroplasty
Three-Part Fractures • Approach • Deltopectoral • Closed Reduction/Pinning • Goals • Tuberosity Fixation • Longitudinal Stability
Hemiarthroplasty • Rarely Indicated • Older Patients • Osteopenic Bone • Fracture-Dislocations • > 40% Impression Defect
Three-Part Fractures Complications • Nonunion • Malunion • Hardware Problems (screw cutout) • AVN
Indications for ORIF of Four-part Fractures Valgus impacted four part with an intact medial soft tissue hinge Four part in a young patient (less than 40)
Indications for Pinning Valgus impacted 4 part proximal humerus fracture • Vascularity preserved by feeding vessels in attached capsule
Valgus Impacted Four PartReduction Maneuver Small incision (2 cm) anterior shoulder Line of fracture usually lies 5 mm lateral to intertubercular groove
Percutaneous PinningReduction Maneuver Valgus Impacted 4 Part
Valgus Impacted Four PartPinning Technique Pin fragments
Valgus Impacted Four Part 47 y.o. female, trip and fall
When to plate? Factors • High energy/low energy • Displacement • 2 part vs 3 or 4 part • Integrity of soft tissue sleeve
46 yo male Rollover dirt bike