Download
1 / 1
10 likes | 103 Views
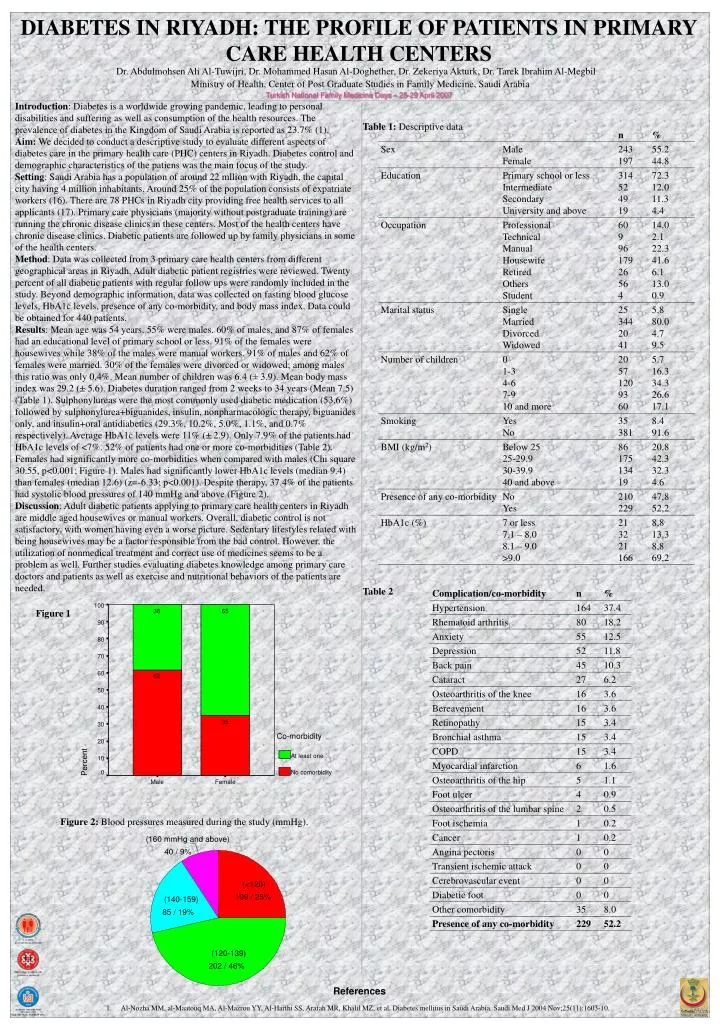
100. 38. 65. 90. 80. 70. 60. 62. 50. 40. 35. 30. Co-morbidity. 20. At least one. 10. Percent. 0. No comorbidity. Male. Female. (160 mmHg and above). 40 / 9%. (<120). 109 / 25%. (140-159). 85 / 19%. (120-139). 202 / 46%.

E N D
100 38 65 90 80 70 60 62 50 40 35 30 Co-morbidity 20 At least one 10 Percent 0 No comorbidity Male Female (160 mmHg and above) 40 / 9% (<120) 109 / 25% (140-159) 85 / 19% (120-139) 202 / 46% DIABETES IN RIYADH: THE PROFILE OF PATIENTS IN PRIMARY CARE HEALTH CENTERS Dr. Abdulmohsen Ali Al-Tuwijri, Dr. Mohammed Hasan Al-Doghether, Dr. Zekeriya Akturk, Dr. Tarek Ibrahim Al-Megbil Ministry of Health, Center of Post Graduate Studies in Family Medicine, Saudi Arabia Turkish National Family Medicine Days – 25-29 April 2007 Introduction: Diabetes is a worldwide growing pandemic, leading to personal disabilities and suffering as well as consumption of the health resources. The prevalence of diabetes in the Kingdom of Saudi Arabia is reported as 23.7% (1). Aim:We decided to conduct a descriptive study to evaluate different aspects of diabetes care in the primary health care (PHC) centers in Riyadh. Diabetes control and demographic characteristics of the patiens was the main focus of the study. Setting: Saudi Arabia has a population of around 22 mllion with Riyadh, the capital city having 4 million inhabitants. Around 25% of the population consists of expatriate workers (16). There are 78 PHCs in Riyadh city providing free health services to all applicants (17). Primary care physicians (majority without postgraduate training) are running the chronic disease clinics in these centers. Most of the health centers have chronic disease clinics. Diabetic patients are followed up by family physicians in some of the health centers. Method: Data was collected from 3 primary care health centers from different geographical areas in Riyadh. Adult diabetic patient registries were reviewed. Twenty percent of all diabetic patients with regular follow ups were randomly included in the study. Beyond demographic information, data was collected on fasting blood glucose levels, HbA1c levels, presence of any co-morbidity, and body mass index. Data could be obtained for 440 patients. Results: Mean age was 54 years. 55% were males. 60% of males, and 87% of females had an educational level of primary school or less. 91% of the females were housewives while 38% of the males were manual workers. 91% of males and 62% of females were married. 30% of the females were divorced or widowed; among males this ratio was only 0.4%. Mean number of children was 6.4 (± 3.9). Mean body mass index was 29.2 (± 5.6). Diabetes duration ranged from 2 weeks to 34 years (Mean 7.5) (Table 1). Sulphonylureas were the most commonly used diabetic medication (53.6%) followed by sulphonylurea+biguanides, insulin, nonpharmacologic therapy, biguanides only, and insulin+oral antidiabetics (29.3%, 10.2%, 5.0%, 1.1%, and 0.7% respectively). Average HbA1c levels were 11% (± 2.9). Only 7.9% of the patients had HbA1c levels of <7%. 52% of patients had one or more co-morbidities (Table 2). Females had significantly more co-morbidities when compared with males (Chi square 30.55, p<0.001; Figure 1). Males had significantly lower HbA1c levels (median 9.4) than females (median 12.6) (z=-6.33; p<0.001). Despite therapy, 37.4% of the patients had systolic blood pressures of 140 mmHg and above (Figure 2). Discussion: Adult diabetic patients applying to primary care health centers in Riyadh are middle aged housewives or manual workers. Overall, diabetic control is not satisfactory, with women having even a worse picture. Sedentary lifestyles related with being housewives may be a factor responsible from the bad control. However, the utilization of nonmedical treatment and correct use of medicines seems to be a problem as well. Further studies evaluating diabetes knowledge among primary care doctors and patients as well as exercise and nutritional behaviors of the patients are needed. Table 1: Descriptive data Table 2 Figure 1 Figure 2: Blood pressures measured during the study (mmHg). References • Al-Nozha MM, al-Maatouq MA, Al-Mazrou YY, Al-Harthi SS, Arafah MR, Khalil MZ, et al. Diabetes mellitus in Saudi Arabia. Saudi Med J 2004 Nov;25(11):1603-10.