Download

1 / 116
1.18k likes | 1.6k Views
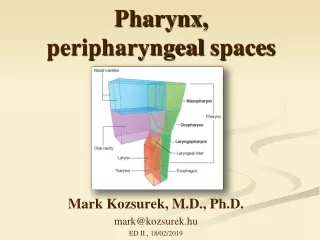
Pharynx. Cruz, Bernadette Anne dC. Flow of Discussion. Anatomy and Physiology Diseases of the Oropharynx Diseases of the Nasopharynx. Diseases of the Oropharynx. Acute Pharyngitis. Etiology and Pathology. Exudate serous thicker or mucoid dry and may adhere to the pharyngeal wall

E N D
Pharynx Cruz, Bernadette Anne dC.
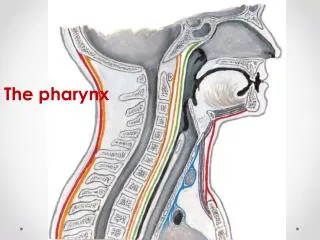
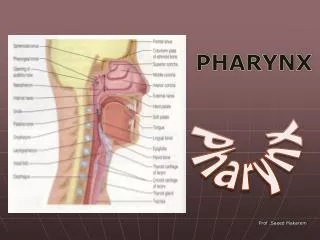
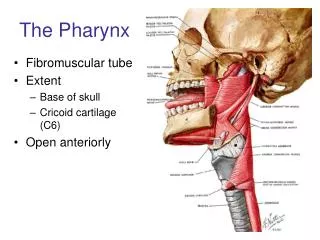
Flow of Discussion • Anatomy and Physiology • Diseases of the Oropharynx • Diseases of the Nasopharynx
Etiology and Pathology • Exudate • serous thicker or mucoid dry and may adhere to the pharyngeal wall • Hyperemia • pharyngeal wall blood vessels become dilated • Small white, yellow or gray plugs form in the follicles or lymphoid tissue
Lateral pharyngitis = lateral wall involvement - lymphoid follicles or plaques on the posterior pharyngeal wall, or localized more laterally, are inflamed and swollen.
Can be due to a viral causative agent • In acute pharyngitis associated with adenopathy in the absence of follicular pharyngitis membrane formation • Vesicle formation on the mucous membrane, ex. Herpes.
Signs and symptoms • Onset • Dryness and scratchiness of the throat • (+) malaise and headache • (+) slight fever
Exudate in the pharynx invariably thickens Difficult, with a rasping, hawking effort and cough Hoarseness Larynx Dysphagia Result of pain, referred pain to the ear, cervical adenopathy, tenderness Pharyngeal wall Reddened Dry, glazed appearance Coating of a mucoid secretion Lymphoid tissue Red and swollen
Normal Acute Pharyngitis
Treatment • Antimicrobials • Shortened course of the disease, decreased incidence of complications • Warm throat irrigations • Supportive care • Adequate fluid intake, light diet, aspirin when indicated
Etiology Acute supppurative bacterial tonsillitis: • ß- hemolytic Streptococcus Group A-most common • Streptococcus viridans • Pneumococci • Staphylococci • H. influenzae • Viral pathogens
Pathology General inflammation and swelling of the tonsil tissue with an accumulation of leukocytes, dead epithelial cells and pathogenic bacteria.
Other pathologic phases that may occur depending on the virulence of organism: • A simple inflammation of the tonsil area • Formation of exudate. • Cellulitis of the tonsil and its surrounding area
Formation of peritonsillar abscess 5. Tissue necrosis
Symptoms • Sore throat • Various degrees of dysphagia • General malaise • Fever- 104°F • Fetid breath • Otalgia • Complications: otitis media Tender cervical adenopathy
Acute Tonsillitis Treatment • Bed rest, adequate fluid intake, light diet • Oral analgesics – control discomfort GARGLES • Adds to a patient’s comfort & influence course of the disease to some extent • 3 glassfuls of gargling solution each time • Every 2 hours • Heat of gargling solution is probably more effective than its medicinal content
Isotonic saline solution, sodium perborate powder which is especially useful in Vincent’s infections or trench mouth ANTIBIOTICS • Treatment of choice • Penicillin – DOC unless organism is resistant or patient is sensitive; erythromycin • Treatment should be continued for a full clinical course, bet 5-10 days • Grp A B-hemolytic strep – maintain adeq antibiotic therapy to reduce possibility of complications such as RHD & nephritis
1. Pharyngeal Tonsil2. Palatine Tonsil3. Lingual Tonsil4. Epiglottis Lingual tonsillitis
The lingual tonsils are at the back of the tongue and cannot be seen by looking in the mouth. Function: guard for infective agents. Composition: Crypts lining by stratified squamousnonkeratinizing epithelium infiltrated with small lymphocytes. Lymphatic nodules LINGUAL TONSILS
LINGUAL TONSILLITIS • Less common than infections of the faucial tonsils due to the absence of the complex crypt arrangement and not as large as the latter. • Rarely, acutely inflamed along with the faucial tonsils. • More common among tonsillectomized patients and adults.
Diagnosis • Examination with a laryngeal mirror or a fiberoptic rhinolaryngoscope will reveal the presence of • acutely inflamed and tender tissue mass with white exudate at the base of the tongue is diagnostic of lingual tonsillitis.
Lingual Tonsillitis Symptoms • Lingual tonsillitis presents with fever, sore throat, dysphagia, muffled voice, and pain at the level of the hyoid bone during swallowing. • The pharynx may appear normal or mildly hyperemic on physical examination.
Lingual Tonsillitis • The anterior neck may be tender at the level of the hyoid bone, and cervical and submandibular adenopathy may be observed. • A patient's voice also may have the classic muffled quality characteristic of severe tonsillar enlargement, but in lingual tonsillitis the uvula and peritonsillar area show no deviation or edema.
TREATMENT • Culture followed by appropriate antibiotic therapy is required. • Lingual tonsillectomy by CO2 laser is performed when medical mgt is not effective.
VINCENT’S OR PLAUT’S ANGINA • An acute necrotizing infection of the pharynx and mouth caused by a combination of fusiform bacilli (Fusiformis fusiformis) and spirochetes (Borrelia vincentii) which are normally present in the oral cavity • Encountered in a limited form without systemic reaction and may be associated with other throat inflammations
CLINICAL MANIFESTATIONS • Commonly seen in young adults • Presents with a unilateral sore throat that increases in intensity over several days with an associated referred earache on the same side. In addition, the patient complains of tender cervical adenopathy and foul breath
Vincent’s Angina A deep well circumscribed unilateral ulcer of one tonsil. The base of the ulcer is gray and bleeds easily when scraped with a swab.
DIAGNOSIS Diagnosis is confirmed by using a gentian violet-stained smear of the pharyngeal exudate, which demonstrates the presence of fusiform bacteria and spirochetes
TREATMENT • Supportive measures • Hydrogen peroxide mouthwash • Penicillin or Clindamycin • Surgical debridement
Diphtheria • Corynebacterium diphtheriae or C. ulcerans • Pharynx is most common site of infection • Occurs more in non-immunized individuals
Diphtheria • Caused by the toxin produced by the organism • Sore throat – most common initial complaint • Nausea, vomiting, dysphagia
Diagnosis • Examination: membrane present over tonsillar area with spread to adjacent structures • Membranes dirty or dark green • May obstruct view of tonsils • Bleeding occurs with elevation of the membrane
Diagnosis • Causative organisms: toxigenic strains of Corynebacterium diphtheriae or C. ulcerans • Smears from nasopharynx and tonsil cultured on MacConkey agar or Loeffler medium • Suspicious strains tested for toxigenicity
Treatment • Two phases • Use of specific antitoxin • Elimination of organism from oropharynx • Antitoxin: test patient first for sensitivity to the serum • 40,000-80,000 units antitoxin diluted in saline, administerd IV
Treatment • Antibiotic treatment: Penicillin or erythromycin • Eliminates carrier state • Repeat culture performed to make sure clearance of organism in the pharynx • Persistent organisms: Long term treatment with erythromycin
Complications • Airway obstruction – tracheostomy • Cardiac failure • Muscle paralysis • Inflammatory process may spread to ears (otitis media), lungs (pneumonia)
Infectious Mononucleosis • Acute Infectious Disease • Fever, Malaise, Somnolence, LN enlargement, Lymphocytosis • Viral (EBV or CMV)
Signs and Symptoms: • Sore Throat • Tonsillitis • Fever • Chills • Malaise • Complaints of feeling tired • LN becomes enlarged and often ulcerates • May block postnasal space
Signs and Symptoms: • Macular Rash 40% • Diffuse and short duration • Increased in patients receiving ampicillin • Splenomegaly in 30% • Jaundice in 5% • Examthem on palate • Short duration of usually less than 48 hours; commonly at the junction of the hard and sof palate
Diagnostics: • CBC • Elevated WBC prodominated by neutrophils • Later followed by lymphocytic leukocytosis • Smear with examination for atypical lymphocytes • “Mono-spot” positive • Heterophil antibody titer exceeds 1:60 • Throat culture to rule-out coexisting beta-hemolytic streptococcal pharyngitis
Treatment: • Symptomatic • Prednisone • For severe obstructive disease • To reduce the ancillary inflammatory process • Patient’s activities should be substantially reduced during the acute phase, with gradual return to normal activities
Complications: • Ruptured Spleen • Guillain-Barre ascending paralysis • CN paralyses