Download
1 / 22
230 likes | 705 Views
Thrombolytic Therapy for Limb Salvage in Severe Frostbite. Or Cold Feet Re-warmed Heart. George R. Edmonson MD Interventional Radiologist St. Paul Radiology Regions Hospital, St. Paul, Minnesota. Lake Mille Lacs. Frostbite.

E N D
Thrombolytic Therapy for Limb Salvage in Severe Frostbite Or Cold Feet Re-warmed Heart George R. Edmonson MD Interventional Radiologist St. Paul Radiology Regions Hospital, St. Paul, Minnesota Lake Mille Lacs
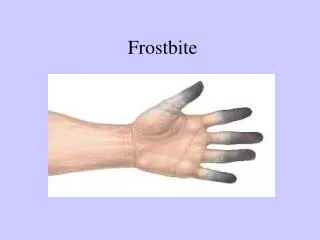
Frostbite • Thermal injury resulting from prolonged exposure to subzero temperatures “Freeze Burns” • Commonly affects the nose, ears, cheeks, hands and feet • May be only superficial or Deep/Severe
Who gets Frostbite • Military • Mountain climbers • Outdoor sportsmen • Stranded travelers • Mentally ill • Drug and/or alcohol intoxicated • The very young or very old
Who gets Frostbite In Minnesota • 36 yr man found outside by police stating “I’m a chicken” • 31 yr man Hunting with friend. Drinking several beers and using crank. Awoke the next morning outside without his gloves. • 90 yr man apparently trying to take out the garbage, found down in the snow • 14 yr boy snuck out of parents house with bottle of liquor and fell asleep outside. Found trying to break in at 5AM • 19 yr man smoking marijuana laced with PCP became paranoid and ran away from his friends • 77 yr man got stuck plowing snow. Lost boot in snow drift
Physiologic Response to Cold • Initial: Small arteries constrict with skin blanching, stinging or burning • Subsequent: shunting occurs bypassing the surface vessels to maintain circulation. Numbness and clumsiness with loss of cold sensation • Final: With further drop in core temp vascular shunting stops and the extremity is allowed to freeze. Cold, grey, bloodless skin
Frostbite: Clinical Findings • Superficial frostbite: limited to skin • Edema after thawing with blisters and pain • Deep frostbite: involves muscles, tendons and bone. Ischemic discoloration. Hemorrhagic blisters common • Recurrent frostbite: blisters often absent • Ultimately nonviable tissue demarcates and sloughs or is amputated
Mechanism of Vascular Injury • Animal Research: Flash frozen rabbit ears • Ice crystals form: primarily in the fluid around the cells • Arteries are initially open after thawing then clot develops due to damage to the cells lining the blood vessels. • Chemical mediators are released which cause intense spasm and inflammation • A Freeze, thaw, then refreeze injury causes ice crystals to form inside the cells destroying them
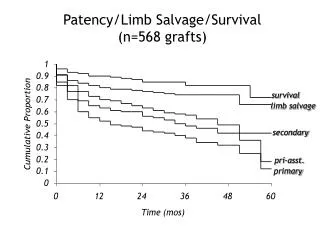
Deep Frostbite Fingers: Outcome without Reopening of Arteries
Rationale for Treatment with TNKase:Plasma Stability and Higher Fibrin Specificity • Primarily small peripheral vessels are occluded • Drugs are infused through catheters in the upper arms or legs • Tenecteplase is degraded more slowly in the bloodstream and binds more firmly to clot when it arrives at the target • Tenecteplase affects the normal clotting proteins less than similar agents therefore bleeding risk may be lower
Our Patient Care Process: Frostbite • Admit to Burn unit via ER. Rapid rewarming of cold extremities. Burn Surgeons assess for severity of injury and blood flow. • May refer for angiography (x-ray dye study) of affected limbs • Diagnostic Arteriography: assess for small vessel occlusion and loss of “distal tuft blush” at the tips of digits • Catheters positioned for simultaneous infusions of treatment drugs into each affected limb. • Blisters and wounds managed in burn unit with debridement or amputation as appropriate
Our Historical Approach • We have been treating frostbite of the extremities with various drugs to dissolve clots and relieve arterial spasm for approx 15 years. • Patients who decline the drugs receive standard supportive care only • Initially: IA Urokinase (UK) with vasodilator papaverine and therapeutic doses of heparin (a “blood thinner”). Generally successful for reopening the arteries over 2-3 days UK was taken off the market. • TPA was being given for acute heart attacks and Reteplase for blood clots in the lungs • TPA: We tried a relatively high dose with heparin. Bleeding complications limited use. • Reteplase: lower dose with low dose heparin used for the next few winters
Frostbite Study Design • FDA and Institutional review board approval obtained. Off label experimental use of drugs. • Open label: Prospective enrollment effort • Up to 10 hospitalized patients ages 18-65 yrs • Drug infusions directly into arteries of the affected limbs • 1-3 limbs treated per patient
Study Endpoints • Angiographic: Flow re-established through occluded vessels to the tips of fingers/toes • Failure to change on 24 hour angiogram i.e. no response to treatment efforts • Clinical: reappearance of distal perfusion • 45 Days: Assess for amputations • Outcome analysis by patient and by limb after drug infusion and at 45 days follow up
Clinical Results: TNK • 6 patients enrolled, all at risk of amputation • 3 patients (4 limbs) responded well with no amputations • 3 patients (6 limbs) had incomplete angiographic response. • 2 improved noticeably then developed infections requiring partial amputation. • 1 patient failed to respond and lost 8 fingers. Thumbs saved • There were no major periprocedural complications
Complete response: Tenecteplase • 20 YO male lost 1 shoe while running through woods from police. Presented with blue right foot with 3 black toes. Initial loss of motor function. • Initial Angiogram: severe vasospasm with no flow to 2nd + 3rd toes. • Right leg Treated overnight: 17 hrs with TNK • Exuberant flow reestablished with distal blush to toes • No amputations on 5 wk follow up. (incarcerated)
Partial Restoration of Bloodflow: 18 yrs male Loss of 1st toe vs. Midfoot amputation
Incomplete response: 18 yrs MaleRight foot Recovery Limited by bone infection
24 Month Reteplase Review (12 pts) • IRB allowed us to look back only 24 months • 10 patients age 14 -77 years (16 limbs) survived to follow up • All treated with various doses of Reteplase and Papaverine • 6 patients recovered with no amputations • 4 patients lost 31 digits at 45 days. 2 had more distal amputation that anticipated • 2 patients excluded from comparison: died 2 weeks after treatment of other causes
Conclusions • Intra-arterial Tenecteplase appears to be safe and effective for reperfusion of limbs devitalized by frostbite • 50% of trial patients avoided amputations which were considered likely without the drug infusions. TNK required less time to reopen arteries than earlier drugs • 5 of 6 patients improved during therapy. • Update: winter 2007-08. • We treated 6 more frostbite patients. • 5 of 6 had complete response. 1 non response • To date: 8 of 12 TNKase Rx patients (68%) saved from amputation • TNK offers a modest improvement over reteplase • Both are much better than traditional treatment
Future Considerations More work is need to understand the causes of failures and optimize the treatment protocol • Increase heparin dose to reduce rethrombosis. We have had no bleeding problems thus far • Add antiplatelet drugs to reduce clot formation • Consider a randomized trial between intravenous and intra-arterial administration of drugs. Two sites have reported some success with high dose IV drug administration.