Download
1 / 32
330 likes | 570 Views
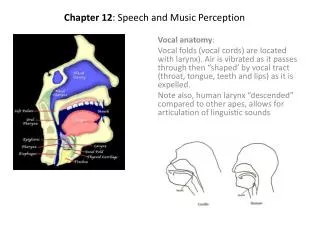
Vocal rehabilitation: The role of the speech-language pathologist. Julianne Mier. Voice Disorders. Voice Disorder- deviation in the speech pattern of an individual, causing the individuals speech to be conspicuous, unintelligible or unpleasant. (Boone, McFarlane, Von Berg, & Zraick, 2010).

E N D
Vocal rehabilitation: The role of the speech-language pathologist • Julianne Mier
Voice Disorders • Voice Disorder- deviation in the speech pattern of an individual, causing the individuals speech to be conspicuous, unintelligible or unpleasant (Boone, McFarlane, Von Berg, & Zraick, 2010)
Voice Disorders • Voice Disorders cause changes to: • Perceptual qualities • pitch, loudness, hoarseness • Acoustic qualities • tremor, frequency breaks, phonation time, etc. • Physiologic qualities • muscle activity, aerodynamics (Boone et. al, 2010)
Voice Disorders • Causes of Voice Disorders • Organic • Neurogenic • Functional (Boone et. al, 2010)
Organic • Voice disorder resulting from a structural change or divergence to the vocal system • Growths or deviations are common • Examples: • granuloma, papilloma, cancer, contact ulcers (Boone et. al, 2010)
Neurogenic • Voice disorder resulting from impairment of the central or peripheral nervous system • Impairment can result from neurotransmitter dysfunction, upper or lower motor neuron lesions, or brain damage • Examples: • vocal fold paralysis, spasmodic dysphonia, dysarthria (Boone et. al, 2010)
Functional • Voice disorders that are secondary to severe emotional problems • Psychological problems are manifested as voice problems • Examples: • conversion aphonia, hoarseness or pitch changes with no physical causes (Boone et. al, 2010)
Treatment • Voice disorders are a medical problem first • Clients must be evaluated by an otolaryngologist prior to treatment • Speech-language pathologist works closely with otolaryngologist, psychologists, nurses, and families (Boone et. al, 2010)
Treatment • Otolaryngolosit determines the structural integrity and function of the voice mechanism • If structural changes or deviations exist, they should first be treated medically (Boone et. al, 2010)
Treatment • Some disorders may require management by medical professionals • Some disorders may be successfully managed by speech pathologists • Some disorder require an integration of multiple approaches (Boone et. al, 2010)
Treatment • Voice treatment is highly individualized • Treatment changes based upon: • cause of problem • maintaining factors • patient motivation • treatment availability • Most importantly treatment is based upon PATIENT PREFERENCE (Boone et. al, 2010)
Treatment • Organic Disorders • Primary treatment is typically medical, dental, or surgical • After primary treatment, speech-language pathologist works to develop the patient’s best possible voice • Work to return the client’s voice to its pre-disordered function and quality (Boone et. al, 2010)
Treatment • Neurogenic • Majority of neurological disorders that impair the voice cannot be cured or eradicated • Primary treatment- medical professionals work to manage the disease • Speech-language pathologists work to maximize vocal function to near normal levels (Boone et. al, 2010)
Treatment • Psychogenic • Voice disorders will not resolve unless the client addresses the underlying issue through counseling or psychotherapy • Speech-language pathologists can provide therapy to help the client experience some vocal improvement prior to completion of counseling (Boone et. al, 2010)
Speech Pathologist’s (SLP) Role: Assessment • Primary objective- evaluate the client’s symptoms and determine a cause of the voice impairment • Secondary objective- patient education and motivation (Boone et. al, 2010)
Speech Pathologist’s (SLP) Role: Assessment • Collect client information: • History of the problem • Medical history • Social history • Complete physical exams as necessary: • Oral mechanism exam • laryngoscopy • Stroboscopy (Boone et. al, 2010)
Speech Pathologist’s (SLP) Role: Assessment • Evaluate the client’s voice: • Observe the client use his or her voice during the assessment • Evaluate the client’s voice in various situations, such as work, home, over the phone, and with strangers • Evaluate the client’s respiratory status • Measure lung volume and air flow • Ask client to count on one breath (Boone et. al, 2010)
Speech Pathologist’s (SLP) Role: Assessment • Obtain acoustic measurements of the voice • Amplitude- the client’s average loudness during conversational speech and the client’s loudness range • Spectral noise- the amount of irregular vibrations in the voice • Maximum phonation time- the length of time a client can sustain a vowel at a comfortable volume • Stoppages- observe and note moments when the client’s vocal folds stop moving, resulting in voiceless speech (Boone et. al, 2010)
Speech Pathologist’s (SLP) Role: Assessment • Quality assessment • Evaluate the clients for abnormal vocal qualities: • hoarse • breathy • tremulous • strained • tension • aphonia (Boone et. al, 2010)
Speech Pathologist’s (SLP) Role: Treatment • SLPs use voice facilitating approaches • Therapy techniques used to target a more optimal vocal response by a client • Used for all causes of voice disorders: organic, functional or psychogenic (Boone et. al, 2010)
Speech Pathologist’s (SLP) Role: Treatment • A large part of therapy is working with the client to find a facilitating approach that helps the client produce the desired vocal response • Therapy is individualized: Two clients with the same diagnosis may require different therapy techniques (Boone et. al, 2010)
Speech Pathologist’s (SLP) Role: Treatment • SLP integrates diagnostic data and behavioral observations to determine the best therapy approach • Medical History • Etiology of Disorder • Acoustic Analysis • Laryngoscopy Results • Client Lifestyle • Client expectations and preferences • Client’s use of harmful behaviors (Boone et. al, 2010)
Speech Pathologist’s (SLP) Role: Treatment • SLP may need to trial different therapy approaches to determine which approach provides the most effective results • Typically multiple approaches are combined to help produced the client’s most natural voice (Boone et. al, 2010)
Treatment by Age • SLP must vary treatment to cater toward the age of the client • Children, adults, and geriatric populations have different conditions that need to be addressed with vocal therapy (Boone et. al, 2010)
Treatment by Age • The most common causes of voice disorders are abuse and misuse and poor breath control (Boone et. al, 2010)
Children • Common problem is hoarseness related to vocal hyperfunction as a result of abuse or misuse • vocal fold thickening, nodules, or polyps • Therapist helps to make the child aware of his or her voice problem • Help the child recognize the situations in which he or she yells excessively or completes other abusive behaviors • Teach the child alternative vocal behaviors and motivate the child to follow these practices (Boone et. al, 2010)
Children • Hard of Hearing or Deafness impacts voice production • The earlier in life the hearing loss occurs, the greater impact it has on the voice • Pitch and nasality problems most often need to be addressed (Boone et. al, 2010)
Adolescents and Adults • Vocal abuse and misuse due to occupations that require excessive talking • Salesmen, teachers, singers • Increased vocal tension, typically related to anxiety • Therapy techniques that target elimination of abuse and vocal relaxation are common (Boone et. al, 2010)
Geriatric • Presbyphonia- gradual weakening of the voice due to aging • Often due to respiration changes and alterations to the musculature of the larynx • SLPs can address respiration changes by teaching proper breathing techniques (Boone et. al, 2010)
Vocal Hygiene & Prevention • All clients can benefit from vocal hygiene: • Drink at least eight 8oz glasses of water a day • Avoid alcohol and caffeine • Take frequent daily “voice breaks” in which you rest your voice for several minutes each time • Avoid abusive behaviors such as yelling or screaming and talking too much/loud • Refrain from throat clearing • Do not whisper, as it is damaging • Keep a normal, relaxed voice when talking/singing • Use amplification when talking to large groups (Boswell, n.d.)
Summary • Voice disorders are prevalent in today’s society • SLP’s work closely with otolaryngologists, as well as other medical professionals to assess and treat clients with voice impairments • Treatments vary depending on the client’s age, gender, disorder, and each client’s unique situation • SLP’s cater treatments toward each client’s individual needs and modify treatments based on the client’s needs and progress during therapy • Proper medical treatment, therapeutic intervention, and counseling are all necessary to remediate the effects of voice disorders and to help the patient achieve a safe and functional voice (Boone et. al, 2010)
Resources • Boone, D. R., McFarlane, S. C., Von Berg, S. L., & Zraick, R. I. (2010). The • voice and voice therapy. Boston, MA: Allyn & Bacon. • Boswell, S. (n.d.) Profiles of prevention: Educating the public on vocal health • and hygiene. Retrieved from http://www.asha.org/SLP/clinical/Educating • the-Public-on-Vocal-Health-and-Hygiene/