Download
1 / 40
450 likes | 507 Views
Explore the intricate anatomy of the eye, common eye infections like conjunctivitis, implicated organisms, routes of entry, and management strategies for various infections in the eye.

E N D
Eye infections Ndonga T.A Msc TID I
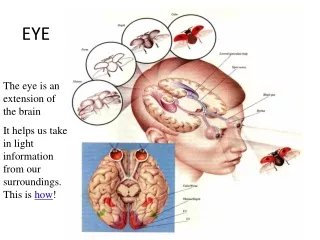
Anatomy • The anterior chamber is the area bounded in front by the cornea and in back by the lens, and filled with aqueous. • The aqueous is a clear, watery solution in the anterior and posterior chambers. • The artery is the vessel supplying blood to the eye. • The canal of Schlemm is the passageway for the aqueous fluid to leave the eye.
Anatomy • The choroid , which carries blood vessels, is the inner coat between the sclera and the retina . • The ciliary body is an unseen part of the iris , and these together with the ora serrata form the uveal tract. • The conjunctiva is a clear membrane covering the white of the eye (sclera). • The cornea is a clear, transparent portion of the outer coat of the eyeball through which light passes to the lens.
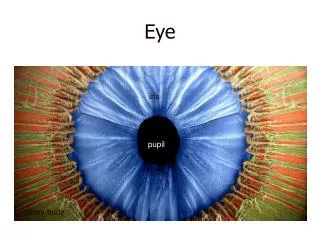
Anatomy • The iris gives our eyes color and it functions like the aperture on a camera, enlarging in dim light and contracting in bright light. The aperture itself is known as the pupil • The lens helps to focus light on the retina. • The macula is a small area in the retina that provides our most central, acute vision. • The optic nerve conducts visual impulses to the brain from the retina. • The ora serrata and the ciliary body form the uveal tract, an unseen part of the iris.
Anatomy • The posterior chamberis the area behind the iris, but in front of the lens, that is filled with aqueous. • The pupil is the opening, or aperture, of the iris. • The rectus medialis is one of the six muscles of the eye. • The retina is the innermost coat of the back of the eye, formed of light-sensitive nerve endings that carry the visual impulse to the optic nerve. The retina may be compared to the film of a camera. • The sclera is the white of the eye. • The vein is the vessel that carries blood away from the eye. • The vitreous is a transparent, colorless mass of soft, gelatinous material filling the eyeball behind the lens.
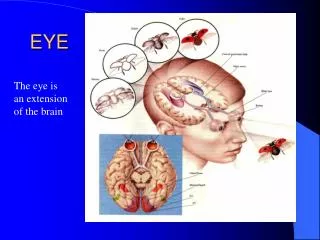
anatomy • The eyeball is protected anteriorly by the eyelids • And contained in the orbit
Normal flora of the eye • Predorminant organisms • Diphtheroids • S.epidermidis • Non hemolytic strep
Eye infections • The infections could be:- • Acute • Chronic • Primary • secondary
conjunctiva • Conjunctivitis is the most common ocular inflammation • Clinical manifestations-hyperemia,secretion –due to exudates of inflammatory cells and fibrin rich edematous fluid-which may be purulent,mucopurulent,fibrinous or serosanguinous depending on the cause. • When the exudate dries ,the eyelids stick together
conjunctiva • The normal transparency may be lost • Papillae may form especially in tarsal conjunctiva • Symptoms include gritty eyes,photophobia,diminished vision and pain
Organisms implicated • *Strep pneumo . C.diphtheria • Strep pyogenes .M.tuberculosis • strep viridians .francisela • *Staph aureus . T.pallidum • *H .influenza .moraxella • *N.gonorrhoea/meningitidis • H.ducreyi . shigella flexeneri • Proteus vulgaris .Y.enterocolitica
organisms • Staph epidermidis • Acinetobacter • Aeromonas hydrophila • Peptostreptococcus • Bartonella • * most common
Routes of entry • Routes of entry-hand to eye -airborne formites -contact with URTIs -contact with genital tract infections -spread from adjacent structures-face and eyelids,sinuses -Hematogenous spread -rare
Determinants of infective agents • Age-neisseriae /chlamydia-newborns • Children-influenza,strep pneumo,staph aureus • Young adults-strep pneumo,staph aureus/epidermidis
Management/control • Mostly self limiting • Px education-hand washing! • Rx-topical gentamicin/tobramycin-gram neg • Neomycin/polymixin-gram pos • Topical quinolones-severe infections • Parenteral ceftriaxone for gonococcal • Erythromycin syrup for chlamydia in neonates/erythromycin ointment.
Cornea • Inflammation of the cornea • Clinically presents as loss of vision,,tearing,photophobia and blepharospasm,ulceration • Symptoms-foreign body sensation,pain
Organisms implicated • Gram pos cocci- gram neg bacilli • *Staph aureus .*pseudomonas • Staph epidermidis . proteus • Strep viridans .klebsiella • Strep pyogenes .serratia • Strep fecalis .E.coli • Peptostreptococcus * most common • *Strep pneumo
organisms • Gram neg coccobacilli gram-positive bacil • Moraxella corynebacterium • Pasturella c.tetani/c.perfringen • Morganella bacillus cereus • Serratia spirochetes • E.coli treponema • Aeromonas borrelia burgdoferi • mycobateria-tb,mac
Routes of entry/predisposing factors • Direct penetration-organisms producing toxins/enzymes/virulent factors-neisseria • Following injury,eyelid abnormalities,tear dysfuntional states,corneal anesthesia • Immunocompromised states • Use of contact lenses
Treatment • Broad spectrum antibiotics used pending lab results-cephalosporins +aminoglycosides • Aminoglycosides can be used synergistically with ticarcillin. • Quinolones-pseudomonas and gram negatives • Use topical antibiotics • Parenteral-severe cases • Steroids??
Endophthalmitis • Most cases develop after intraocular surgery-cataract surgery. • Organisms involved-microflora • Clinically-decreased visual acuity,pain,hypopion,hyperemia
organisms • Staph aureus .E.coli • Staph epidermidis .H.influenza • Strep pneumo .klebsiella • Bacillus cereus .moraxella • Corynebacteria spp .proteus • Listeria .pseudomonas • N.meningitidis .s.typhimurium • Acinetobacter .serratia • Enterobacter .clostridium • Propiono bacterium acnes treponema pallidum • Actinomyctes israeli .m.tuberculosis/leprae
Treatment • Is according to culture and sensitivity • Iv antibiotics-3G cephalosporins • Intravitreal vancomycin-s.aureus • Sx-vitrectomy • Steroids??
Periocular infections • These involve orbit and cellular adnexa • Principal periocular structure susceptible to infections are eyelids ,the components of lacrimal apparatus and the orbit.
Eyelids • Inflammation of the lid margins-blepharitis • Often chronic and bilateral • Two types-anterior-staphylococcal -posterior-meibominitis Organisms Staphaureus,epidermidis,pseudomonas,proteus,moraxella .Mascara used has been implicated
Eyelids • Erysipelas-acute cellulitis –strep pyogenes,staph aureus-invasion of subcutaneous after trauma • Hordeolum-internal/external depending on glands involved-staph implicated • Internal-meibomian gland infection • External-stye infection of glands of zeis sebaceous gland of eye lids
Lacrimal apparatus • Produce the aqueous component of tear film • Canaliculitis-chronic inflammation of canaliculi-by propionibacterium,actinomyces • Dacrocystitis-inflammation of lacrimal sac-streppneumo,staphaureus,pseudomonas,chlamydia,h.influenza in children • Clinically-epiphora
Lacrimal app • Dacroadenitis-inflammation of main lacrimal gland-staph,strep,tuberculosis-chronic
Orbit and carvenous sinus • Cellulitis-pre septal anterior orbit septum and post septal-orbital contents • Serious-loss of sight and spread to carvenous sinus leading to thrombosis and death,
causes • Spread from contiguous structures like sinuses,dental,intracranial infections • Direct innoculation after puncture wounds • Retained foreign bodies-sutures • After surgery • After fractures • Sequelae of dacrocystitis • Bacteremia in kids H.influenza,E.fecalis
organisms • Staph aureus • Strep pyogenes • Strep pneumo • Clostridia • H.influenza-<5s • Tb-hematogenous spread
Clinical • Evidence of trauma-bleedng,fever,lid edema and rhinorrhoea. • Pain,headache,loss of vision • Tenderness,black eye,proptosis
Treatment • Blepharitis-Topical –bacitracin,erthromycin • Steroids-reduce inflammation • Hordeolum-warm compresses and sytsemic antibiotics if multiple or no response I&D if not responding to rx • Canalliculitis-antibiotic irrigation with penicillin G • Dacrocystitis-oral penicillin+warm compresses
treatment • Dacroadenitis-systemic antibiotics • Cellulitis-cloxacillin,oxacillin,cephalexin • Clindamycin for gram neg • Iv antibiotics orbital cellulitis
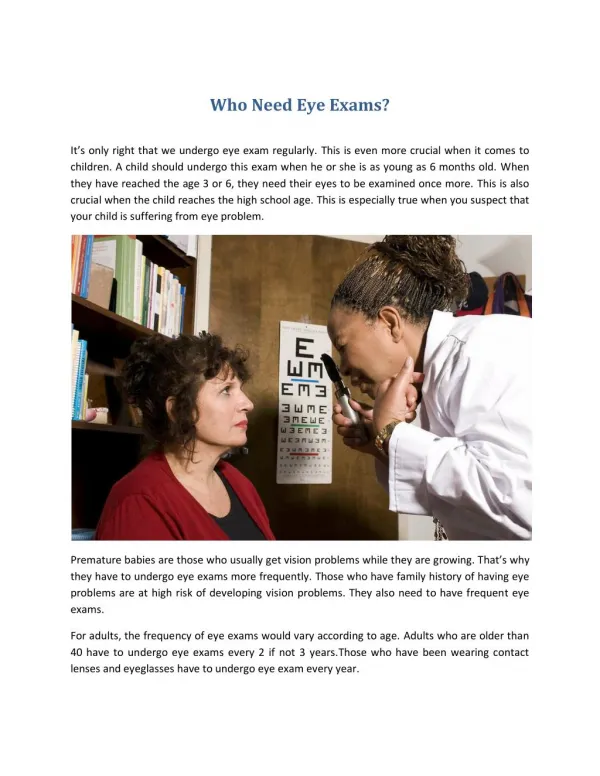
Approach to diagnosis of eye infections • Mostly clinical diagnosis • Slit lamp examination • Swabs –conjunctiva, abscesses etc • Cultured on BA • Swab each anaesthetized eye separately • Can also do scrapings-cornea • Vitreous/aqueous humour aspiration- endophthalmitis
diagnosis • Gram stain • ELISA • Dna/pcr-chlamydia • Fluorescent microscopy • u/s,ct,MRI for cellulitis