Download
1 / 37
370 likes | 649 Views
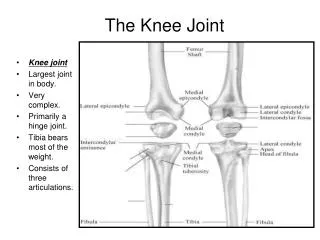
Knee Problems ?. Sam Rajaratnam Consultant Orthopaedic Surgeon Eastbourne DGH, Horder Centre, Esperance Hospital, Eastbourne. Questions & Dilemmas. Physiotherapy or Orthopaedic Surgeon ? MRI or Xray ? Which views ? Operate or Not ? Total Knee replacement or Partial ?

E N D
Knee Problems ? Sam Rajaratnam Consultant Orthopaedic Surgeon Eastbourne DGH, Horder Centre, Esperance Hospital, Eastbourne
Questions & Dilemmas • Physiotherapy or Orthopaedic Surgeon ? • MRI or Xray ? Which views ? • Operate or Not ? • Total Knee replacement or Partial ? • Can we afford it ?? • Which hospital ? Fracture/Knee injury clinic/ Elective setting
Not mutually exclusive We work in teams Physio – good for weak muscles/extra articular problems/ secondary stiffness Surgeon – can deal with intra-articular pathology Physio vs Surgeon
Curable • Arthritis • Instability • Cartilage tears • Intra-articular pain
Things that may be treated conservatively • Chondromalacia patellae • Tendinosis • Bakers cysts
X-Ray or MRI • Xrays – Much more useful for Osteoarthritis (probably avoid Primary care MRI’s) • MRI - useful for Meniscal tears or ligament injuries
Xrays Much better for arthritis(Antero-medial wear – Most common pattern (60 %) . Very Painful)
Isolated patello-femoral wear • Pain on walking up & down stairs • No problem walking on flat ground • Patella can “lock” or “catch” • Knee giving way
Lateral Osteoarthritis • Knee Gives way • “Knock Knee” • Deformity can progress rapidly • Often required total knee replacement (remember – disease of flexor surface)
Cartilage surface defects • MRI Poor at diagnosing these • Look for articular surface tenderness & effusion
3. Diagnose Acute Ligament Injuries • MCL • ACL • PCL • MPFL
Reminder - Acutely injured knee • Intra-articular injuries present with pain and swelling • Extra-articular ligament injuries present with pain
MCL Injury Tenderness, stress testing Grade I Local tenderness+slight or no laxity Grade 2 Local tenderness+laxity with endpoint. Grade 3 Complete rupture No endpoint.
ACL History • running (high velocity) • change of speed and direction • “snap” or “pop” • pain • immediate swelling (<4hours) • unable to play on • CLINICAL FINDINGS • Swelling is haemarthrosis • Restricted range of motion usually due to ACL stump or muscular spasm • almost never meniscal tear locking joint in acute primary injury • LIGAMENT EXAMINATION • LACHMAN • PIVOT SHIFT • ANTERIOR DRAWER TESTS
Arthroscopic View • Torn ACL • POST RECONSTRUCTION
Day Surgical Arthroscopic Hamstring ACL - Accelerated Rehabilitation Key Changes • Pre ACL Rehab • Patient education • Improved technique • Ice cold saline infusion • Advanced Local Blockade • Physiotherapy services Key to good results Early reconstruction before meniscal damage has occurred
4. Patella Dislocation - MPFL Traumatic • May heal • May require MPFL Repair Spontaneous • Bad bony alignment • Soft Tissue laxity
Cartilage Repair • Suitable for 15 – 55 year old • Discrete area of chondral damage • Stable knee (no ligament instability) • Medial femoral condylar defects , Trochlea groove, Patella • Various techniques available
Can Britain afford it ? • Probably not………….but as secondary care clinicians, the decision is easy • Treat the patient in front of you as best you can…..
Thank you – Any Questions ? Sam Rajaratnam Consultant Orthopaedic Surgeon Eastbourne DGH Horder Centre, Esperance Hospital, Eastbourne