Download
1 / 146
1.48k likes | 1.64k Views
Radiation Safety for Licensed Practitioners Using Fluoroscopic X-Ray Equipment. Summary: To Minimize Patient Dose. ONLY X RAY WHEN YOU ARE PREPARED TO VISUALLY INTERPRET THE FLUORO IMAGE ON THE MONITOR. Minimize x-ray beam on-time Fluoro at low frame rates Fluoro at low dose rate settings

E N D
Radiation Safety for Licensed Practitioners Using Fluoroscopic X-Ray Equipment
Summary: To Minimize Patient Dose • ONLY X RAY WHEN YOU ARE PREPARED TO VISUALLY INTERPRET THE FLUORO IMAGE ON THE MONITOR. • Minimize x-ray beam on-time • Fluoro at low frame rates • Fluoro at low dose rate settings • Minimize amount of ciné/DSA • Utilize distance • Keep the patient skin far from the x-ray tube • Keep the image receptor close to the patient • Empty patient bladder of iodine for pelvic procedures • Cone-in to the smallest practicable beam size • Minimize patient dose by spreading it over a larger area by small changes in projection
Summary: To Minimize Worker Dose • Each worker must wear a lead apron • Each worker must wear their radiation badge (if one has been assigned) • Each worker should stay as far from the patient as possible • The operator should • ONLY X RAY WHEN THE PHYSICIAN IS PREPARED TO VISUALLY INTERPRET THE FLUORO IMAGE ON THE MONITOR. • Minimize x-ray beam on-time • Fluoro at low frame rates • Fluoro at low dose rate settings • Minimize amount of ciné/DSA • Empty patient bladder for pelvic procedures • Cone-in to the smallest practicable beam size
Objectives (I) • Be aware of the effects of high x-ray doses on the skin of patients in fluoroscopy • Review physics of x-ray imaging • Production of x rays • Interactions of x rays • Image receptors • Radiation dose • Review methods to minimize patient dose • Review ways to minimize occupational dose
Objectives (II) • Review State regulations requiring radiation training of physicians doing fluoroscopy • Review Joint Commission requirements for a Sentinel Event for patient skin doses. • Review ASLMC Policy #219, written to address this issue. • Review biological effects of radiation exposure.
X ray imaging delivers radiation dose to the patient • Countless patients over the past century have benefited from their physician being able to visualize function and anatomy using x-ray imaging. • All x-ray imaging delivers radiation dose to the patient. There are two concerns from this dose: • Any dose increases the risk to the patient of developing cancer. This small increase in risk must be greatly outweighed by the benefit of enhanced diagnostic information. • If the radiation dose is sufficiently high, the skin of the patient will be damaged.
Skin damage from prolonged x-ray imaging in interventional procedures The effect of ~20,000 mGy from 3 angioplasty procedures. at 6 weeks at 18 months The effect of the patient draping his arm on the lateral x-ray tube in a biplane room. at 3 weeks at 12 months
Skin damage from prolonged x-ray imaging in interventional procedures These must be considered unacceptable consequences of medical imaging!
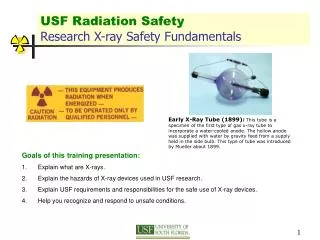
FDA and Joint Commission Requirements • By 1994 the FDA had called attention to the problem of skin burns from fluoroscopy, and recommended methods for minimizing skin dose. • In 2006 FDA required new x-ray fluoro units to monitor patient skin dose. • In 2007 the Joint Commission deemed any fluoroscopic skin dose in excess of 1,500 rad (15,000 mGy) to be a Sentinel Event. • This presentation will assist you in understanding • How to minimize your patient’s dose and thereby avoid such effects. • How to minimize your occupational dose while performing procedures
State of Wisconsin Requirements Operators* of fluoroscopy equipment are required to be trained in radiation safety per Wis DHS 157.76(11)(e) * Those whose foot is on the switch to activate the x-ray beam.
State of Wisconsin Requirements The State authorizes only licensed practitioners to independently use fluoroscopic x-ray equipment. This includes Physicians, Podiatrists Nurse practitioners, Physician Assistants Radiologist’s Assistants Dentists, Chiropractors licensed in the state of Wisconsin
Review the physics of x-ray production • X rays are produced as a result of electrical phenomena in a vacuum x-ray tube • The x-ray tube contains • A wire filament called the cathode • A metal-coated disk called the anode • The filament is heated with electrical current, causing negatively charged electrons to be ejected off the surface of this hot filament. • A very high voltage called the kV is applied from the filament to the anode. This accelerates the electrons to high energy.
X Ray Imaging Physics • X rays are produced in an x-ray tube, and the beam of x-rays is put onto the patient • Those parts of the patient that are thick, dense or of high atomic number, absorb more x rays than surrounding tissues. • The x-ray beam transmitted through the patient is imaged by an image receptor. Image Receptor X-ray Beam X-ray Tube
The x-ray tube and tube housing X-Ray Tube The x-ray tube is a vacuum glass tube holding two electrodes. Tube Housing The tube housing is a lead-lined can holding the tube and insulating oil
The x-ray tube has two electrodes Anode (tungsten layer on a graphite disk) Filament
X-ray tube operation The filament is heated with electrical current The heat causes electrons to be ejected into the vacuum of the tube
X-ray tube operation Apply kV (e.g. 80 kV = 80,000V) across tube Electrons accelerated to anode - +
X-ray tube operation: kV and mA The kV gives energy to each electron The flow of electrons is the mA - +
X-ray tube operation As the electrons smash into the tungsten-surfaced anode, they create x rays by a process called bremsstrahlung
X-ray tube operation X Rays in the Primary Beam The Focal Spot is the area on the anode where x-rays are produced
Bremsstrahlung creates x rays over a wide range of energies.
Higher kV = more x rays of all energies Higher kV = higher energy x rays
Changing the mA causes a proportional change in the number of x rays of all energies Double the mA, you double the number of x rays of all energies
The x-ray beam The x rays leaving the x-ray tube constitute the primary x ray beam
The x-ray beam – noise/mottle The number of x rays per area per time in the primary x ray beam is inherently random. This causes the response in the image to be random, and the image to contain quantum uncertainty (or mottle or noise.) If there are n x-rays per area per time in the beam, the noise or randomness is proportional to So, more x rays minimizes the noise. (But more x rays increases the dose!) To cut the noise in half, you need to increase the number of x rays by 4!
Image Noise Few x rays = noisy image = poor definition of small, low contrast objects. But, small dose. 1 x-ray per 10 pixels 1 x-ray per pixel Many x rays = little noise =better definition of small objects at low contrast. But, large dose. 1,000 x-rays per pixel 10 x-rays per pixel
Image Noise Optimum x ray imaging occurs when the desired diagnostic information is obtained with the lowest possible dose. For example, if the task here was to “identify the subject in these photos,” we can do this from this noisy image just as well as we can from one with 1,000 times the number of x rays! 1 x-ray per pixel 1,000 x-rays per pixel 10 x-rays per pixel
The x-ray beam filter The x ray beam passes through a metal “filter” that removes low energy x-rays (These low energy x-rays would not have penetrated the patient anyway, and would not have contributed to the image. They would have just added dose to the patient.)
The most modern x-ray systems change the beam filter automatically. Thin or low density patients (requiring fewer x rays incident on the patient) are imaged with the 0.3 mm copper filter. Thick or dense patients (requiring more incident x rays in order to have sufficient penetration to the image receptor) are imaged without the copper filter. Portable C-arm units generally use fixed 2.5 mm Al filtration.
A thicker filter = fewer low energy x rays = a more penetrating x-ray beam A thicker filter = less patient skin dose.
The X-Ray Unit Operates in Two Modes • Fluoroscopy • Real-time (constantly updated) imaging • Can utilize x-ray beams that are continuously-on, or pulsed • Uses much lower dose per frame than cine fluorography • Cine fluorography or “acquisition” in Interventional Labs • String of radiographic snap shots of the patient, often with temporal image subtraction to achieve angiography (“DSA” = digital subtraction angiography) • Uses high radiation dose for each frame • Generates low noise images • Better definition of small, low contrast objects • Typically 15 frames are acquired per second for adult cardiac imaging
Image Receptor Types • The x-ray beam transmitted through the patient is intercepted by the Image Receptor, which absorbs x rays and creates the image • Two types of image receptors are in use • Image Intensifier • Flat panel digital radiography detectors • Both types can be equally good! Image receptor Transmitted x-ray beam patient X-ray tube
Image Intensifier • The Image Intensifier is a large vacuum tube. • Operation: • X rays from the patient are absorbed at one end in the “input phosphor” & create light • The light hits an adjacent “photocathode” layer, which converts light to electrons in the vacuum • A high voltage (HV) accelerates the electrons to the other end of tube • Electrons are absorbed in an “output phosphor,” which recreates the visible image • The visible image is bright because • Energy is given to each electron by the HV (called “flux gain”) • The image is smaller than the x-ray beam, and the light emitted off the small-area output phosphor creates a brighter image
Image Intensifier Visible light image Output phosphor (electrons converted to light) Anode (+25kV accelerates electrons) Vacuum tube Photocathode (convert light electrons) e- e- e- Input phosphor (converts x-rays light) X rays transmitted through patient
Image Intensifier • The visible image at output phosphor of the image intensifier is seen by a video camera • video pickup tube, or, • CCD (charged coupled device) • These convert the light image into an electronic video or computerized image Video camera Image intensifier tube
Flat panel digital radiographic detector • A flat panel DR detector directly converts the x-ray beam transmitted through the patient into tiny pieces (pixels) of a computer image • Two types of flat panel detectors are in use: • Cesium Iodide (CsI) layer on amorphous silicon (aSi) plate • X rays are absorbed in the CsI, & light from CsI is converted into a pixel’s signal in the aSi • Amorphous selenium (aSe) • Plate of aSe absorbs x rays and generates electrical charge, which is converted into a pixel’s signal
Modern computer image display • Modern fluoroscopy and cine fluorography images are • Stored in a computer format, typically at 1024 pixels across 1024 pixels vertically • Displayed on a computer monitor • Image processing software is often available to optimize the x-ray image • Contrast enhancement, edge sharpening or smoothing, temporal averaging to minimize noise
Pulsed vs Continuous Fluoroscopy • Continuous fluoroscopy • X-ray beam is on continuously as long as the foot pedal is activated • The image receptor is read and the image on the monitor updated in real-time (30 times per second) • Pulsed fluoroscopy may be available • X-ray beam is on for short bursts, each lasting ~3 to ~10 msec • Short burst needed to freeze patient motion • The rate of these pulses is user-selectable: • Real time: 30 frames per sec (fps), or pulses per sec (pps) • Less than real time: • 15 fps • 7.5 fps • etc
Pulsed vs Continuous Fluoroscopy • Patient dose (and dose to those in the room) may be reduced using pulsed fluoroscopy • 30 frames per sec (real time) = same dose as continuous fluoro • 15 fps = 1/2 the dose of continuous • 7.5 fps =1/4 the dose of continuous • The price is poorer temporal resolution, since the image is not updated as often
Pulsed Fluoroscopy: low frame rate = low dose 30 fps Fluoro images X ray pulses Time 33 msec 15 fps Fluoro images X ray pulses Time 67 msec
Pulsed Fluoroscopy: low frame rate = low dose 30 fps Fluoro images X ray pulses Time 33 msec 15 fps ½ THE DOSE! Fluoro images X ray pulses Time 67 msec
Use Last Image Hold (LIH) in Fluoroscopy • “Last Image Hold” on a fluoro system displays the last acquired fluoro image even after the x-ray beam is off • “Last Image Hold” has been found to be useful in allowing the physician to interpret the information on the fluoro monitor without additional radiation exposure. Fluoro monitor shows the same image X ray pulses Time
Fluoroscopy Dose Rate Settings • Modern x-ray units may allow the user to fluoro at various radiation dose rates (by adjusting mA and filter) • GE: • “Low Detail” (= lower dose rate) vs • “Normal Detail” (= higher dose rate) • Siemens: • “Fluoro –” (= lower dose rate) • “Fluoro normal” • “Fluoro +” (= higher dose rate) • Higher dose rate fluoro • Generates images with less noise • But, delivers higher patient and operator radiation doses
C-arm Fluoroscopy Dose Rate Settings • Modern C arm x-ray units may allow the user to fluoro at various radiation dose rates • GE / OEC C arms: • “Normal Fluoro” (typical 30 fps live fluoro) • Pulsed Fluoro (8 pulses per sec) = 25% of the dose rate of Normal Fluoro • “Low Dose” Fluoro = 40% of the dose rate of Normal Fluoro • “High Dose Rate Fluoro”typically gives ~85% MORE dose than Normal Fluoro
Mini-C-arm Fluoroscopy Dose Rates • Mini-C arm x-ray units • Operate the x-ray tube at very low mA and not more than 81 kV • Have small x-ray beams, and so generate relatively little scatter • However, they still generate x-rays and must be used with caution X-ray tube X-ray beam Image Intensifier
The Radiation Intensity Varies with Distance from the Source • Consider a source of radiation, for example • The x-ray tube focal spot (for the primary beam), or • Scatter generated in the patient • The intensity (dose) of radiation varies with distance from the source as 1/distance2 X-ray source Dose meter distance
25 mGy 200 cm 400 mGy 50 cm The Radiation Intensity Varies with Distance from the Source: Examples 100 mGy 100 cm
100 mGy 100 cm 400 mGy 50 cm The Radiation Intensity Decreases with Increasing Distance from the Source 25 mGy 200 cm Doubling the distance cuts the x-ray intensity to 1/22 = 1/4 of its original value