Download
1 / 67
690 likes | 895 Views
MRI SPINE /KNEE. DR, Mohamed El Safwany , MD. Intended learning outcome. The student should learn at the end of this lecture MRI aspects of spine and knee. TISSUE COLOURS. Water and pathology: White on T2, dark on T1. Pathology stays white on FLAIR, water doesn't. TISSUE COLOURS.

E N D
MRI SPINE /KNEE DR, Mohamed El Safwany, MD.
Intended learning outcome The student should learn at the end of this lecture MRI aspects of spine and knee.
TISSUE COLOURS • Water and pathology: • White on T2, • dark on T1. • Pathology stays white on FLAIR, water doesn't
TISSUE COLOURS • Fat: • white on T1 and T2 • dark on STIR and out of phase
TISSUE COLOURS • Hematoma: varying with time
TISSUE COLOURS • Bone Marrow: normally fatty • white on T1 • White on T2 • replaced with edema or other pathology • (dark on T1) • Bone cortex, stones, and ligaments • dark on everything • Contusion is white
TISSUE COLOURS • Tumor: hypervascular (neovascularity): • white with gadolinium
Approach to protocols • T1 -MRI with dark fluid • T2 -MRI with white water, inflammation • cartilage is black • STIR- T2 with dark fat • Proton Density - cartilage is grey • can suppress the fat • Gadolinium enhanced - with fat suppressionT1 • bright blood • dark fat • Pathology bright
Magnetic resonance imaging (MRI) of the spine • A noninvasive procedure to evaluate different types of tissue, including • the spinal cord • intervertebral disks • spaces between the vertebrae through which the nerves travel • distinguish healthy tissue from diseased tissue.
Magnetic resonance imaging (MRI) of the spine • The cervical, thoracic and lumbar spine MRI should be scanned in individual sections. • The scan protocol parameter like e.g. the field of view (FOV), slice thickness and matrix are usually different for cervical, thoracic and lumbar spine MRI, but the method is similar.
Magnetic resonance imaging (MRI) of the spine • The standard views in the basic spinal MRI scan to create detailed slices (cross sections) are • sagittal T1 weighted and T2 weighted images over the whole body part • transversal (e.g. multi angle oblique) over the region of interest with different pulse sequences according to the result of the sagittal slices. • Additional views or different types of pulse sequences like fat suppression, fluid attenuation inversion recovery (FLAIR) or diffusion weighted imaging are created dependent on the indication.
Indications: • Neurological deficit, evidence of radiculopathy, caudaequina compression • Primary tumors or drop metastases • Infection/inflammatory disease, multiple sclerosis • Postoperative evaluation of lumbar spine: disk vs. scar • Evaluation of syrinx • Localized back pain with no radiculopathy (leg pain)
Contrast enhanced MRI • Delineate infections, malignancies • show a syrinx cavity • support to differentiate the postoperative conditions. After surgery for disk disease, significant fibrosis can occur in the spine. This scarring can mimic residual disk herniation. • Magnetic resonance myelography evaluates spinal stenosis and various intervertebral discs can be imaged with multi angle oblique techniques.
Advanced open MRI devices are developed to perform positional scans in the position of pain or symptom (e.g. Upright™ MRI formerly Stand-Up MRI).
Contraindications • MRI systems use strong magnetic fields that attract any ferromagnetic objects with enormous force. • Caused by the potential risk of heating, produced from the radio frequency pulses during the MRI procedure, metallic objects like wires, foreign bodies and other implants needs to be checked for compatibility. • High field MRI requires particular safety precautions. • In addition, any device or MRI equipment that enters the magnet room has to be MR compatible. • MRI examinations are safe and harmless, if these MRI risks are observed and regulations are followed.
Safety concerns in magnetic resonance imaging include: • The magnetic field strength; • possible 'missile effects' caused by magnetic forces; • the potential for heating of body tissue due to the application of the radio frequency energy; • the effects on implanted active devices such as cardiac pacemakers or insulin pumps; • magnetic torque effects on indwelling metal (clips, etc.); • the audible acoustic noise; • danger due to cryogenic liquids; • the application of contrast medium;
MRI Safety Guidance • It is important to remember when working around a superconducting magnet that the magnetic field is always on. • Under usual working conditions the field is never turned off. • Attention must be paid to keep all ferromagnetic items at an adequate distance from the magnet. • Ferromagnetic objects which came accidentally under the influence of these strong magnets can injure or kill individuals in or nearby the magnet, or can seriously damage every hardware, the magnet itself, the cooling system.
MRI Safety Guidance • The doors leading to a magnet room should be closed at all times except when entering or exiting the room. • Every person working in or entering the magnet room or adjacent rooms with a magnetic field has to be instructed about the dangers. • This should include the patient, intensive-care staff, and maintenance-, service- and cleaning personnel, etc..
MRI Safety Guidance • Leads or wires that are used in the magnet bore during imaging procedures, should not form large-radius wire loops. • The patient’s skin should not be in contact with the inner bore of the magnet.
MRI Safety Guidance • The outflow from cryogens like liquid helium is improbable during normal operation and not a real danger for patients
MRI contrast • The safety of MRI contrast agents is tested in drug trials and they have a high compatibility with very few side effects. • The variations of the side effects and possible contraindications are similar to X-ray contrast medium, but very rare. • In general, an adverse reaction increases with the quantity of the MRI contrast medium and also with the osmolarity of the compound.
Cervical Spine 1 – Basic • • Indications • o Disc disease, pain, radiculopathy • • Sequences • o Sag T1 FSE/TSE • o Sag T2 FSE/TSE • o Ax T2 FSE/TSE • o Ax TOF GRE • • Optional • o Cor T1 FSE/TSE • o Cor T2 FSE/TSE • For scoliosis, tethered cord and Neurofibromatosis, add coronal
Cervical Spine 2 – with contrast • • Indications • Tumor, Infection, MS, Syrinx, Transverse myelitis • • Sequences • Sag T1 FSE/TSE • Sag T2 FSE/TSE • Ax T1 FSE/TSE • Ax T2 FSE/TSE • Sag T1 +C FSE/TSE FS • Ax T1 +C FSE/TSE FS • • Optional • Cor T1 FSE/TSE • Cor T2 FSE/TSE
Cervical Spine 3 – Trauma • • Indications • o Trauma • • Sequences • o Sag T1 FSE/TSE • o Sag T2 FSE/TSE • o Sag IR T2 FSE/TSE • o Ax IR T2 FSE/TSE • o Ax T2 FSE/TSE • Can add sag T2 GRE to r/o hemorrhage
Thoracic Spine 1 - Basic • • Indications • Disc disease, pain, radiculopathy • • Sequences • Sag T1 FSE/TSE • Sag T2 FSE/TSE • Ax T1 FSE/TSE • Ax T2 FSE/TSE • • Optional • Cor T1 FSE/TSE • Cor T2 FSE/TSE
Thoracic Spine 2 – with contrast • • Indications • Tumor, Infection, MS, Syrinx, Transverse myelitis • • Sequences • Sag T1 FSE/TSE • Sag T2 FSE/TSE • Ax T1 FSE/TSE • Ax T2 FSE/TSE • Sag T1 +C FSE/TSE FS • Ax T1 +C FSE/TSE FS • • Optional • Cor T1 FSE/TSE • Cor T2 FSE/TSE
Thoracic Spine 3 – Trauma • • Indications • Disc disease, pain, radiculopathy • • Sequences • Sag T1 FSE/TSE • Sag T2 FSE/TSE • Sag IR T2 FSE/TSE • Ax T2 FSE/TSE • • Optional • Ax GRE • Cor T1 FSE/TSE • Cor T2 FSE/TSE • Can add Sag GRE to rule out hemorrhage
Routine L-Spine MRI • Degenerative spine • Sagittal T1 SE, • Sagittal T2 FSE, • angled axial PD/T2 FSE, • Angled T1 stacked axials L3 to S2. • No IV contrast.
L-Spine MRI • Trauma L-Spine MRI • Sagittal T1 SE, • Sagittal FSEIR, • Axial T2 FSE with fat sat. • Target axials to abnormality. • No IV contrast. • Post-Op L-Spine MRI • Sagittal T1 SE, • Sagittal FSEIR, • Axial T2 FSE with fat sat. • Target axials to abnormality at level of surgery • IV contrast. • Can add Sag GRE to rule out hemorrhage
Osteomyelitis, Discitis • pre-contrast: • Sagittal T1 SE, • Sagittal T2 FSE, • Axial PD/T2 FSE, • contrast: Gd (0.1 mmol / kg to max of 20 cc) • post-contrast: • Sagittal T1 SE, • Axial T1 SE
Spine Survey • • Indications • Metastases, Non-localized infection, acute myelopathy / cord compression • • Sequences • Sag T1 FSE/TSE • Sag T2 FSE/TSE • Ax T1 FSE/TSE • Ax T2 FSE/TSE • Sag T1 +C FSE/TSE FS • Ax T1 +C FS (region of interest) • • Optional • Cor T1 FSE/TSE • Cor T2 FSE/TSE • • Comments • sagittal images to determine where to obtain axial images
MRI KNEE • Common Indications • Knee pain • Knee instability • Knee mass
First Ask • Is there a mass?______ When did you first discover the mass?_______________________ • Does the problem relate to a recent injury? YES NO DATE_____________________ • Where does the knee hurt ( FRONT - BACK - INSIDE - OUTSIDE )? • Have you had surgery on your knee? YES NO DATE__________________________ • Have you had an x-ray? • If “mass” then schedule in early morning with Radiologist monitoring. Patient may need gadolinium • Otherwise schedule anytime. • Instruct patient to bring x-rays if available.
Patient Preparation: • · Fill out safety screening and clinical information form • · Vitamin E capsule on the site of symptoms and on any masses • · Measure distance left or right from centerline of magnet
Coil: Extremity. Slightly externally rotate the foot by about 10-15 degrees to stretch the anterior cruciate ligament. • Pack some cushions around the knee to help it stay motion-free. A small cushion under the ankle helps to keep the leg straight. • Landmark: inferior region of patella. • Patient Positioning: Supine, feet first.
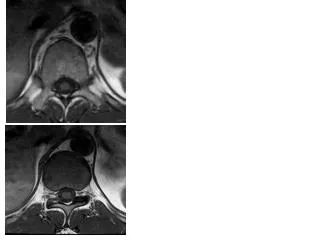
Series 1: Axial Proton Density • Series 2: Sagittal Proton Density • Oblique to the intercondylar notch • Include all of medial and lateral menisci. Subcutaneous fat medial and lateral to knee joint may be excluded. If more slices are required, increase TR.