Download
1 / 18
180 likes | 342 Views
1 st Line Disease Modifying Therapies. Disease modification. Therapeutic considerations Long-term efficacy of treatments Benefits vs risks Side effect profiles Co morbidity Concomitant medication Potential benefits of combination therapy Patient needs and views. Immunomodulators.

E N D
Disease modification Therapeutic considerations • Long-term efficacy of treatments • Benefits vs risks • Side effect profiles • Co morbidity • Concomitant medication • Potential benefits of combination therapy • Patient needs and views
Immunomodulators • Immunomodulators • glatiramer acetate • beta interferons • Proven effectiveness in reducing relapse rates and severity • May slow accumulation of disability • Maximum benefits from: • Use in RRMS • Early and continuous treatment, some evidence for use in CIS • Prescribing in accordance with ABN Guidelines ABN Guidelines for the treatment of multiple sclerosis with Beta Interferons and Glatiramer Acetate ABN Nov 2009
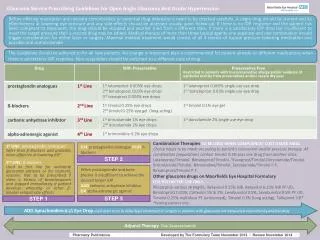
Glatiramer acetate Under ABN Guidelines and Risk Sharing Scheme May be used for relapsing-remitting MS for patients who can walk 100m having had two relapses in previous 2 years ABN Guidelines for the treatment of multiple sclerosis with Beta Interferons and Glatiramer Acetate ABN Nov 2009
Beta interferons Under ABN Guidelines and Risk Sharing Scheme Interferon beta 1a & b May be used for relapsing-remitting MS for patients who can walk 100m having had two relapses in previous 2 years Interferon beta 1b May be used for patients with secondary progressive MS who can walk 10m aided or unaided who have relapses within the progression of their MS ABN Guidelines for the treatment of multiple sclerosis with Beta Interferons and Glatiramer Acetate ABN Nov 2009
Cytokine production • MMP production • BBB disruption • CNS influx GA Th2 Mechanisms of Action Centrally BBB Periphery IFN b IFN receptor Activation Passive decrease of CNS inflammation? IFN b Glatiramer Acetate • Active bystander regulation • Neuroprotection Th2 bias
Glatiramer acetate • Mode of action differs from interferons • Changes proinflammatory Th1 cells into anti inflammatory Th2 cells • Well tolerated • Reduces relapse rate by 30% in RRMS • Reduces MRI burden of disease • Reduces black hole evolution • Long-term relapse data – 15 years Johnson KP et al. 1995 Neurology. 45(7):1268-1276 Johnson KP et al. 1998 Neurology. 50(3):701-708 Comi GC et al. 2001 Annals of Neurology. 49(3):290-297 Filippi M et al. 2001 Neurology. 57:731-733 Ford CC et al. 2006 Multiple Sclerosis. 12:309-320
Glatiramer acetate • Effect on disability progression - much debate • Effect on neuroprotection - much debate • Does not exacerbate depression • 25 % find associated improvement in fatigue • No routine blood tests necessary Wolinsky JS et al. 2002 Neurology. 59:1284-1286 Ziemssen T et al. 2002 Brain. 125:2381-2391 Filippi M et al. 2001 Neurology. 57:731-733 Copaxone Summary of Product Characteristics 2009
Beta interferons • Interferon are naturally occurring proteins and play a crucial role in the functioning of the immune system • They are produced by a variety of cells in response to microbial stimuli • Block T cell activation • Inhibit the action of gamma-interferon and induce other substances to suppress the level of immune activity • Anti viral • Reduce relapse rate by around 30% The IFNB Multiple Sclerosis Study Group. 1993 Neurology. 43:655-661 Jacobs LD et al. 1996 Annals of Neurology. 39:285-294 The PRISMS Study Group. 1998 Lancet. 352:1498-1504
Beta interferons • Reduce severity of relapses • Rapid suppression of MRI detectable disease activity (within 4 weeks) • Controversy continues regarding effect on disability progression, • likely to be greatest where relapses are dominant feature • As of August 2006, all products licensed for early use, however, use in CIS is still not indicated under the current ABN guidelines (2009). ABN Guidelines for the treatment of multiple sclerosis with Beta Interferons and Glatiramer Acetate Nov 2009 The IFNB Multiple Sclerosis Study Group. 1993 Neurology. 43: 655-661 Jacobs LD et al. 1996 Annals of Neurology. 39: 285-294 The PRISMS Study Group. 1998 Lancet. 352: 1498-1504 Jacobs LD et al. 2000 New England Journal of Med Medicine. 343: 898-904 European Study Group on Interferon-1b in Secondary Progressive MS. 1998 Lancet. 352: 1491-1497 Comi G et al. 2001 Lancet. 357: 1576-1582
Neutralising Antibodies (NAbs) • All immunomodulators create antibodies • Antibodies developed by the beta interferons may neutralise effect of drug • Patients who develop NAbs are 60% more likely to experience relapses • Likely to occur 6-12 months after commencing therapy • It is suggested that all beta interferon patients should be tested for NAbs at 12-24 months • Ongoing debate about the influence of Nabs on treatment Sorensen PS et al. 2005 European Journal of Neurology. Nov;12(11):817-27. The PRISMS Study Group and the University of British Columbia MS/MRI Analysis Group. 2001 Neurology. 56(12):1628-36
Comparable relapse rates Retrospective study undertaken in Argentina Carra A et al. 2003 Eur J Neurology. 10: 671-676 Khan 0 et al. 2002 CNS Drugs. 16(8): 563-578 Haas J et al. 2003 Presented at the AAN Annual Meeting, March 29-April 5, 2003 Honolulu, Hawaii
Minimising injection site reactions • The key to minimising injection site reactions is rotation, rotation, rotation. • Injection sites should be observed at all clinical reviews regardless of the therapy. Prevention and Management of injection site reactions during therapy with glatiramer acetate. Samantha Colhoun British Journal of Neuroscience Nursing, 3(1)24 – 28 Jan 2007.
Interference with T-cell activation Yes Yes Decrease in Th1 and enhancement of Th2 cytokines Yes Yes Induces Th2 response Yes No Inhibits T-cell/BBB transmigration* No Yes CNS effects Yes No Neuroprotection Yes Indirect Antibodies Inert (Beneficial?) Neutralizing Glatiramer Acetate vs. Beta interferons Glatiramer Acetate Beta-Interferons *Critical differences Adapted with permission from Dhib-Jalbut S 2002 Neurology. 58:S3-S9
When to change / discontinue treatment • This varies from centre to centre • There is no standardised pathway • No reduction in relapse rate • Increased severity of relapses • Development of neutralising antibodies • Intolerable side effects/injection site reaction • Treatment discontinued in accordance with ABN Guidelines (2009)