Download
1 / 40
540 likes | 2.64k Views
Placenta Previa. R.L. 33 y/o G4P3 (3002), PU 37 3/7 weeks AOG Married Filipino Roman Catholic. General Data. scheduled Cesarean section. Reason for consult. (-) hypertension (-) diabetes mellitus (-) bronchial asthma (-) thyroid disease No known allergies

E N D
R.L. • 33 y/o • G4P3 (3002), PU 37 3/7 weeks AOG • Married • Filipino • Roman Catholic General Data
scheduled Cesarean section Reason for consult
(-) hypertension • (-) diabetes mellitus • (-) bronchial asthma • (-) thyroid disease • No known allergies • s/p LTCS IIIx (Ix for CPD) Past Medical History
nonsmoker and alcoholic beverage non-drinker Personal and Social History
(+) hypertension – father • (+) bronchial asthma – mother • (-) diabetes mellitus • (-) cancer Family History
Menstrual History Menarche – 11 y/o Interval – regular, 28 days LMP: October 25, 2009 Duration – 2-3 days PMP: Sptember 2009 Amount – 3-4 ppd, fully-soaked Symptoms – (+) dysmenorrhea, day 1 • Sexual History Coitarche – 21 y/o; single sexual partner; (-) dyspareunia, postcoital bleeding; (-) history of STI • Contraception Use: (+) use of OCPs x 2 months (2006); no IUDs • Latest PAP smear was in June 2010: Normal results Gynecologic History
G4P3 (3002) • G1 (2000) – delivered to a live full term baby boy via primary LTCS for cephalopelvic disproportion attended by doctor – Fabella Hospital, BW 2kg, neonatal death x 10 days, neonatal sepsis secondary to meconium aspiration • G2 (2001) – delivered to a live full term baby girl via repeat LTCS attended by doctor – SLMC • G3 (2005) – delivered to a live full term baby boy via repeat LTCS attended by doctor – SLMC • G4 – present pregnancy Obstetric History
4 months AOG FPNCU • 5 months AOG (+) vaginal bleeding, ~10 ppd fully soaked • No hypogastric abdominal pain, no uterine contractions, no foul smelling vaginal discharge, no passage of meaty tissue, no fever • Sought consult • TVS: placenta previa totalis • Prescribed Isoxilan tablet (Duvadilan) TID x 7 days History of Present Illness
6 months (+) vaginal bleeding, 5 ppd/fully soaked • Same associated signs and symptoms • took Isoxilan tablet TID x 3 days (self-medicated) • did not seek consult • Few hours prior to admission repeat TVS • placenta previa totalis to consider placenta accreta • scheduled Cesarean section
General • Denies fever or malaise • HEENT • Denies headache, blurring of vision, hearing problems, epistaxis, tooth or throat pain • Pulmonary • Denies cough or dyspnea • Cardiovascular • Denies palpitations or chest pain • Gastrointestinal • Denies diarrhea and constipation • No nausea and vomiting, anorexia Review of Systems
Urinary • Denies dysuria, frequency, nocturia • Endocrine • Denies polyuria, polydipsia, tremors • Hematopoietic • Denies easy bruisability • Musculoskeletal • Denies myalgia or arhtralgia • Neurologic/Psychiatric • Denies change in sensorium or behavior
Conscious, coherent, not in cardio-respiratory distress, intermittently in pain • BP: 110/70mmHg CR: 80/min, regular RR: 20/min, regular T: 36.8oC • Skin: no suspicious lesions • Head: skull normocephalic, atraumatic • Eyes: pink palpebral conjunctivae, anictericsclerae • Neck: supple neck, with no palpable neck mass, no neck vein engorgement Physical Examination
Lungs: symmetrical chest expansion, no rib retractions, clear and equal breath sounds • Heart: adynamicprecordium, normal rate, regular rhythm, no murmurs • Abdomen: globular abdomen, (+) midline scar; FH 33cm, EFW 3255g, FHT 140bpm; LM 1: breech LM 2: fetal back on maternal left LM 3: unengaged • Non tender abdomen, no rigidity • Full and equal pulses, no cyanosis Physical Examination
External pelvic examination: no lesions, redness, excoriations, hyper/hypopigmentations • IE deferred Pelvic Examination
Subjective • 33 yoG4P3 (3002), PU 37 3/7 weeks AOG • (-) HPN, s/p LTCS IIIx (Ix for CPD) • Non smoker • RPNCU since ~4mos AOG, no maternal illnesses, with 2 episodes of vaginal bleeding in the 2nd trimester. • ~5 mos (+) vaginal bleeding, ~300 mL • No hypogastric abdominal pain, no uterine contractions, no foul smelling vaginal discharge, no passage of meaty tissue, no fever • TVS: placenta previa • Isoxilan tablet (Duvadilan) TID x 7 days • (+) vaginal bleed ~150ml @ 6 mos AOG • Few hours PTA, TVS was done which showed: • Placenta previa totalis t/c placenta accreta scheduled CS Salient Features
Objective • Conscious, coherent, not in cardio-respiratory distress, intermittently in pain • BP: 110/70mmHg CR: 80/min, regular RR: 20/min, regular T: 36.8oC • Abdomen: globular abdomen, (+) midline scar; FH 33cm, EFW 3255g, FHT 140bpm; LM 1: breech LM 2: fetal back on maternal left LM 3: unengaged • No abdominal tenderness, no rigidity Salient Features
G4P3(3002) PU 37 3/7 weeks AOG, cephalic, not in labor, placenta previa totalis, t/c placenta accreta previous LTCS IIIx (Ix for cephalopelvic disproportion) Clinical Impression
Placenta Previa • Abruptio Placenta • Spontaneous Abortion • Cervicitis Differential Diagnosis
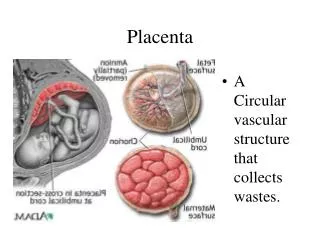
Placenta Previa is a condition where the placenta lies low in the uterus and partially or completely covers the cervix. DEFINITION
Total placenta previa • the internal os is covered completely by placenta • Partial placenta previa • the internal os is partially covered by placenta • Marginal placenta previa • the edge of the placenta is at the margin of the internal os • Low-lying placenta • the placenta is implanted in the lower uterine segment such that the placental edge does not reach the internal os, but is in close proximity to it • Vasaprevia • the fetal vessels course through membranes and present at the cervical os (uncommon, associated with higher rate of fetal death Four degrees of abnormalities
Placenta previa affects about 1 in 200 pregnant women (Iyasu et al., 1993). Incidence
Placenta previa is more common in women who have had one or more of the following: • Increasing maternal age • Multiparity • Prior cesarean delivery • Surgery on the uterus • Smoking • Multiple gestation (larger surface area of the placenta) Risk Factors
Placenta accreta, placenta increta or placenta percreta • Secondary to the poorly developed decidua on the lower uterine segment. Placenta Previa is associated with:
Placenta accreta -- Abnormal adherence of the placenta to the myometrial wall, with absence of decidua basalis.
Placenta increta--placenta attaches deep into the uterine wall and penetrates into the uterine muscle, but does not penetrate the uterine serosa
Placenta percreta-- Placental villi penetrate myometrium and through to uterine serosa.
Painless hemorrhage (most characteristic) • Due to tearing of placental attachments during the formation of the LUS or during cervical dilatation • Bleeding occurs at the implantation site as the uterus is unable to contract adequately and stop the flow of blood from the open vessels. • Hemorrhage persists after delivery because of the LUS contracts poorly so it cannot constrict the torn vessels. May also be due to lacerations in the cervix and LUS following manual removal of adherent placenta Clinical Findings:
Placental implantation is initiated by the embryo adhering in the lower uterus. • With placental attachment and growth, the developing placenta may cover the cervical os. • However, it is thought that a defective decidualvascularization occurs over the cervix, possibly secondary to inflammatory or atrophic changes. Pathophysiology
Diagnosis can seldom be established by clinical examination unless a finger is passed thru the cervix the placenta is palpated. Such examination is never permissible because even the gentlest examination may cause torrential hemorrhage. • Such examination is rarely necessary since placental location can be obtained by sonography. Diagnosis
The most useful and inexpensive study is transvaginal ultrasonographythat provides >95% accuracy in identifying a placenta previa • An alternative would be transabdominal ultrasonography that can be 95% accurate; however, the false-positive and false-negative rates can range from 2-25%. Imaging Studies
MRI may be used for planning the delivery in that it may help identify placenta accreta, placenta increta, or placenta percreta. These invasive placental abnormalities are more common (eg, placenta accrete occurs in up to 0.2% of pregnancies) due to the increase in cesarean deliveries, advancing maternal age, hypertensive disease, smoking, and placenta previa cases. Imaging Studies
MRI is no more sensitive in diagnosing placenta accreta that ultrasonography, but it may be superior for the posterior placenta accreta or the more invasive increta and percreta. Imaging Studies
Preterm fetus but with no active bleeding: • Close observation • In some cases, prolonged hospitalization is ideal but the patient is discharged after bleeding has stopped and fetus is assessed to be healthy. • If bleeding persists, preparation for immediate surgery is indicated. Management
Additionally, tocolytics may also be considered in cases of minimal bleeding and extreme prematurity to administer antenatal corticosteroids. If more than one episode of bleeding occurs during gestation (at viability or >24 wk), the clinician should consider hospitalization until delivery given the increased potential for placental abruption and fetal demise. Management
Cesarean delivery is necessary in practically all cases of placenta previa. • Poorly contractile nature of the LUS there may be uncontrollable hemorrhage following placental removal. • Oversew the implantation site with 0-chromic sutures • Bilateral uterine artery ligation or internal iliac artery ligation • Tightly packing the LUS with gauze • If bleeding persists hysterectomy Management