Download
1 / 78
1.24k likes | 4.16k Views
Atrial Septal Defects. Ali Mahajerin Non-Invasive Cardiology Conference December 12, 2007. Introduction. Atrial septal defect (ASD) is detected in 1 child per 1500 live births, and accounts for 5-10% of congenital heart defects.

E N D
Atrial Septal Defects Ali Mahajerin Non-Invasive Cardiology Conference December 12, 2007
Introduction • Atrial septal defect (ASD) is detected in 1 child per 1500 live births, and accounts for 5-10% of congenital heart defects. • ASDs make up 30-40% of all congenital heart disease detected in adults (second only to bicuspid aortic valve). • ASDs occur in women 2-3 times as often as men.
Introduction • ASDs can occur in different anatomic portions of the atrial septum. • ASDs can be isolated or occur with other congenital cardiac anomalies. • Functional consequences of ASDs are related to the anatomic location of the defect, its size, and the presence or absence of other cardiac anomalies.
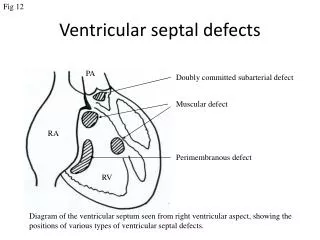
Classification • Primum ASD • Secundum ASD • Sinus venosus defects • Coronary sinus defects • (Patent foramen ovale)
Primum ASD • Make up ~15% of all ASDs. • Occur if the septum primum does not fuse with the endocardial cushions, leaving a defect at the base of the interatrial septum that is usually large. • Usually not isolated – primum ASDs are typically associated with anomalies of the AV valves (such as cleft mitral valve) and defects of the ventricular septum (VSDs) or a common AV canal.
Secundum ASD • Make up ~70% of all ASDs. • Occur twice as often in females. • Typically located within the area bordered by the limbus of the fossa ovalis. • Defects vary in size, from <3 mm to >20 mm.
Secundum ASD • May be associated with other ASDs. • Multiple defects can be seen if the floor of the fossa ovalis (AKA valve of the foramen ovale) is fenestrated. • Ten to twenty percent have a functional mitral valve prolapse • May be related to changing LV geometry associated with RV volume overload
Sinus venosus ASD • Make up ~10% of ASDs. • Characterized by malposition of the insertion of the SVC or IVC straddling the atrial septum. • Often associated with anomalous pulmonary venous return – the RUL/RML pulmonary veins may connect with the junction of the SVC and RA in the setting of a superior sinus venosus ASD.
Coronary Sinus Septal Defects • Less than 1% of ASDs • Defects in the inferior/anterior atrial septum region that includes the coronary sinus orifice. • Defect of at least a portion of the common wall separating the coronary sinus and the left atrium – AKA “unroofed coronary sinus” • Can be associated with a persistent left SVC draining into the coronary sinus.
Patent Foramen Ovale • Not truly an “ASD” because no septal tissue is missing. • Oxygenated blood from the IVC crosses the foramen ovale in utero. • At birth, the flap normally closes due to • Reduced right heart pressure and PVR • Elevated LA pressure. • Flap fusion is complete by age two in 70-75% of children; the remainder have a PFO.
Pathophysiology of ASDs • Not an issue in utero – flow is occurring through the foramen ovale. • After birth, generally LA pressure > RA pressure: • PVR falls (lungs have expanded) • SVR rises (placenta has been removed) • Pulmonary venous blood flow is increased; all flows into LA • Left-to-right shunting occurs across the ASD – this depends on the size of the defect, the relationship of PVR and SVR, and the compliance of RV and LV. • Brief R-to-L shunting also occurs during cardiac cycle in children (during inspiration, LA pressure decreased and RA pressure increased) – causes mild neonatal cyanosis.
Pathophysiology of ASDs • Generally L-to-R flow across ASD • Occurs mainly in late ventricular systole and early diastole; some augmentation during atrial systole. • The volume of pulmonary blood flow is greater than systemic blood flow because of this circuit. • Qp/Qs can be as high as 8:1, though in asymptomatic young adults is usually 2:1 to 5:1.
Pathophysiology - consequences • Right-sided volume overload leads to dilation of right-sided chambers. • Main pulmonary arteries dilate, and pulmonary vascularity is increased. • Eventual development of pulmonary hypertension. • RV function can become decreased. • Eisenmenger syndrome, with RV failure and right-to-left shunting of blood.
Clinical Manifestations • Children may be asymptomatic; may have easy fatigability, exertional dyspnea. Underdeveloped, more prone to respiratory infections. • Most patients with shunt flow ≥ 2:1 will be symptomatic and require correction by age 40. • Exercise intolerance, fatigue, dyspnea, and overt heart failure are the common presentations in adulthood. • Risk of atrial arrhythmias increases with age and PA pressure. • Pulmonary hypertension and Eisenmenger syndrome – 50% occurrence in unoperated ASDs.
Physical Exam Findings • Wide, fixed splitting of S2 (delayed closure of pulmonic valve with reduced respiratory variation) • Midsystolic pulmonary flow or ejection murmur • Usually over 2nd intercostal space • Peaks in early-to-mid systole, ends before S2 • Palpable RV heave • Usually no audible murmur across the ASD • Eisenmenger’s sequellae: cyanosis, clubbing • Murmur of MR if cleft MV also present (primum ASD)
EKG Findings • Right atrial enlargement d/t vol overload (tall P wave) • RVH – RAD, RSR’ in V1, R>S in V1. • Atrial tachyarrhythmias – a.fib, atrial flutter • AV delay – often with primum ASD in association with LAFB and RBBB (the rim of an ostium primum defect is near the His bundle).
Chest X-Ray Findings • Dilation of RA and RV • Enlarged main pulmonary arteries and pulmonary vessels, without redistribution to apical vessels. • Left atrial enlargement if associated mitral regurgitation.
Echocardiography and ASDs • Some clues to the presence of ASD: • Abrupt discontinuity of the septum, and slight thickening at its termination • RA enlargement, RV enlargement/dilation • Dilated pulmonary arteries • Increased flow velocity in the PA and across TV • Paradoxical motion and diastolic flattening of the ventricular septum • TTE is usually definitive in secundum ASDs. • TEE will help with sizing defects, and identifying sinus venosus defects.
Two-Dimensional TTE Apical four-chamber view • Can often see ostium primum ASD in this view. • Shadowing and echo dropout (especially in the area of the fossa ovalis) may lead to false positives. Subcostal view • Often more reliable - can visualize entire atrial septum. • Sensitivity for ASD detection: • Primum ASD: 100% • Secundum ASD: 89% • Sinus venosus ASD: 44%
Color Doppler TTE • Can confirm the presence of the ASD, estimate the defect size, and evaluate the efficacy of surgery. • Flow extends from mid-systole to mid-diastole; second phase of flow coincident with atrial systole. • May have brief R-L shunting. • Usually not a high velocity jet. • Must avoid confusing the low-velocity shunt flow with normal venous and AV valve flow.
Contrast Echo • Administer agitated saline contrast through IV. • Apical four-chamber view is usually optimal. • Bubbles in the LA suggests right-to-left shunting at the atrial level if 3 bubbles within 3 cardiac cycles following complete opacification of the RA. Delayed bubbles may be due to pulmonary AVMs – may be less phasic in appearance. • Large ASDs may have nearly continuous shunting, but smaller ASDs may be more phasic with respiration. • May see “negative contrast effect” if mainly left-to-right shunt.
Contrast Echo - PFOs • Often a small, hemodynamically insignificant left-to-right shunt present in PFO based on the unsealed overlap of foraminal valve. • The shunt is often phasic with respiration. • Maneuvers such as Valsalva or cough, which transiently increase R heart pressure, may allow the occult R-to-L shunt component of a PFO to become evident.
Transesophageal Echo • TEE is superior to TTE in visualizing the interatrial septum and identifying all types of ASDs. • With contrast or Doppler, TEE can detect any brief right-to-left shunting that may occur with transient increases in right-sided pressure. • TEE is much more sensitive than TTE for detection of left-to-right shunt as negative right atrial contrast (93% vs. 58% in one study). • TEE can detect flow through multiple ASDs.
Transesophageal Echo • Estimation of defect size using the diameter of the Doppler color flow jet correlates with surgical findings. • Since ASDs are not necessarily round, TEE helps with determining both their size and shape. This is especially important when percutaneous closure is being contemplated. • TEE is often used when contrast echo suggests shunting, but a defect can’t be visualized on TTE. The TEE then helps to differentiate between a PFO and a true ASD. • TEE is particularly helpful for diagnosis of sinus venosus ASDs.
Can provide excellent details regarding: Shunt flow Defect size Pulmonary venous return Large sinus venosus ASD Qp/Qs 2.7 Anomalous return of right upper pulmonary vein to RA Increased RV cavity size, normal RV function Cardiac MR
Cardiac MR • Qp/Qs = 2.0 • Dilated RA, increased RV cavity size, evidence of RV volume overload • Normal pulmonary veins
Cardiac MR • Severely increased RV size, mild RV free wall hypokinesis, volume overload, dilated RA • No significant AR or MR, normal LV • Sinus venosus ASD with significant L-to-R shunt • Qp/Qs 3.03 • Normal pulmonary venous return – the right upper pulmonary vein enters the LA at its junction with the RA and empties in the region of the ASD.
Cardiac MR • Large primum ASD, Qp/Qs 2.3; possible associated membranous VSD. • Normal LV cavity size; LVEF 66%, effective forward LVEF 43%. Increased RV size, RVEF 51%. • Main PA diameter 37 • Paradoxical interventricular septal motion c/w RV volume overload • Mod-severe MR with likely cleft anterior leaflet of MV • Biatrial enlargement
Estimation of Shunt Flow Ratio • Operative closure of an ASD traditionally recommended when the ratio of pulmonary blood flow to systemic blood flow (Qp/Qs) is greater than 1.5:1 or 2:1. • Can estimate Qp/Qs from TTE measurements using Pulsed Doppler echocardiography. Cardiac MR is also useful for further assessment of Qp/Qs ratio. • Correlation between Doppler imaging and cardiac catheterization techniques for this measurement is good.
Estimation of Shunt Flow Ratio • First measure stroke volume through each valve: Stroke Volume (Q) = CSA x VTI • Left-sided stroke volume is measured from LVOT (diameter measured in parasternal long axis view). • Maximum Doppler flow velocity apical to aortic valve (VTILVOT) taken in apical four-chamber view. • Right-sided velocity time integral (VTIPA) measured in PA well before bifurcation. • PA diameter measured at the same level as VTIPA.
Estimation of Shunt Flow Ratio • Substitution into stroke volume ratio gives: Qp/Qs = (PAdiam)2 x VTIPA ------------------------------------- (LVOTdiam)2 x VTILVOT • Diameters of LVOT and PA are squared – exact measurement of these values is especially important. • PA diameter can be difficult to assess in some patients; this is the term that is most often responsible for inaccurate estimates of the shunt ratio.
Natural History of ASDs • Most ASDs <8mm close spontaneously in infants. • Spontaneous closure is unusual in children and adults; defects often become progressively larger. • Most patients with a significant shunt flow ratio (Qp:Qs > 2:1) will be symptomatic and require closure by age 40. • Increasing size of the ASD may preclude percutaneous closure.
Natural History of ASDs • Life expectancy is not normal, though many patients live to advanced age. • Natural survival beyond age 40-50 is <50%. • The attrition rate after age 40 is ~6% per year. • Advanced pulmonary hypertension seldom occurs before the third decade. • Atrial fibrillation is a late complication; stroke is a potential complication of ASD (ongoing investigation into this issue).
Indications for Defect Closure • 1.) Symptoms • Exercise intolerance, fatigue, dyspnea, heart failure • Atrial tachyarrhythmias? • Occur in 20% and often the presenting symptom • Not an indication by itself (incidence may not be reduced after surgery).
Indications for Defect Closure • 2.) Defect Size and Qp/Qs • Larger ASDs impose a greater hemodynamic burden on the RV. • In the absence of pulmonary hypertension, Qp/Qs is closely correlated with the size of the ASD. • Qp/Qs > 2:1 is a well-established indication, though many authors advocate 1.7:1 or even 1.5:1. • AHA recommends a threshold Qp/Qs ≥ 1.5:1, but these guidelines exclude patients > 21 years of age. • Canadian Cardiac Society recommends Qp/Qs >2:1, or >1.5:1 in the presence of reversible pulmonary hypertension.
Surgical Closure • Median sternotomy is the traditional approach; minimally invasive approaches are emerging. • Pericardial or Dacron patches are used. • Primary closure of the defect is not recommended. • Can repair other defects at the same time (such as cleft mitral valve if primum ASD). • Intraoperative TEE useful to assess adequacy of repair; can also assess for any new TR or MR that is occurring from tension of the repair.
Surgery: Efficacy • Does surgery still benefit patients who are older at the time of diagnosis? • Attie et al. prospectively evaluated 473 pts. over age 40 diagnosed with secundum ASDs, randomized to surgery vs. medical Rx • Mean age 51 • Median follow-up of 7.3 years. • Qp/Qs ratio 2.3 ± 0.7 • Primary endpoints = death, PE, major arrhythmia, embolic CVA, recurrent pulmonary infection, functional class deterioration, or heart failure. Attie F, et al. JACC 2001; 38(7): 2035-42.
Composite primary endpoint occurred more frequently with medical than surgical therapy (21 vs 11 percent, H.R. 2.0). • Overall mortality not statistically different, but there was a nonsignificant trend toward higher sudden death rate with medical treatment (2.9 vs 0.9 percent). • Multivariate analysis (adjusted for age at entry, mean PASP > 35 mmHg, previous atrial tachyarrhythmia, and C.I. < 3.5 L/m2) had a significantly higher mortality with medical management (H.R. 4.1).
Surgery: Efficacy • Konstantinides et al. retrospectively evaluated 179 patients with isolated ASDs diagnosed after age 40 (91% secundum, 3% primum, 6% sinus venosus) • Compared 84 pts. (47%) who underwent surgery vs. 95 pts. (53%) who were treated medically. • Mean age 54±7 years for the surgery group, 57±10 years for the medical therapy group. • Mean follow-up period 8.9±5.2 years • Cardiac symptoms reported in 94% at presentation. • “The decision not to operate was based on the judgment of the cardiologists and cardiac surgeons involved in each case.” Konstantinides S, et al. NEJM 1995; 333(8): 469-73.
Surgery: Efficacy • Multivariate analysis revealed a reduced mortality from all cause in the surgical group (relative risk 0.31; 95% C.I. 0.11-0.85). • Ten-year survival rate was 95% in surgical group, 84% in medically treated group. • Surgical treatment prevented functional deterioration (11% vs. 34%, relative risk 0.21, 95% C.I. 0.08-0.55) and improved functional status (32% vs. 3%, p=0.002). • Incidence of new atrial arrhythmias or stroke was not significantly different. Konstantinides S, et al. NEJM 1995; 333(8): 469-73.
Long-Term Surgical Outcomes • Surgery before the age of 25 yields in 30-year survival rates comparable to age- and sex-matched controls. • At 25-40 years of age, surgical survival is reduced, though not significantly if PA pressures are normal. • If PASP > 40 mmHg, late survival is 50% less than control rates, though life expectancy in surgically treated older patients is better than that of medically treated patients. • No benefit of surgery in reducing the incidence of AF, though the patient’s age at the time of closure is the most important predictor of the development of atrial arrhythmias.