Download
1 / 18
180 likes | 283 Views
X-Rays. Kunal D Patel Research Fellow IMM. The 12-Steps. }. 1 : Name 2 : Date 3 : Old films 4 : What type of view(s) 5 : Penetration 6 : Inspiration 7 : Rotation 8 : Angulation 9 : Soft tissues / bony structures 10 : Mediastinum 11 : Diaphragms 12 : Lung Fields.

E N D
X-Rays Kunal D Patel Research Fellow IMM
The 12-Steps } • 1: Name • 2: Date • 3: Old films • 4: What type of view(s) • 5: Penetration • 6: Inspiration • 7: Rotation • 8: Angulation • 9: Soft tissues / bony structures • 10: Mediastinum • 11: Diaphragms • 12: Lung Fields Pre-read } Quality Control } Findings
Reviewing these areas Heart • Size • Shape • Silhouette-margins should be sharp • Evidence of stents, clips, wires and valves • Diameter (>1/2 thoracic diameter is enlarged heart) • Mediastinum • Width? • Contour? • Lung fields • Apices • Lobes and fissures • USE SILHOUETTES • CP angles • Diaphragm • Gastric bubble • NOTE normal pleura are NOT visible
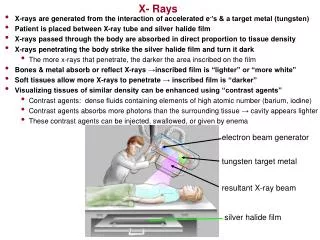
FINDINGS! • A = Airway: are the trachea and mainstem bronchi patent; is the trachea midline? • B = Bones: are the clavicles, ribs, and sternum present and are there fractures, lytic lesions? • C = Cardiac silhouette: is the diameter of the heart > ½ thoracic diameter (enlarged)? • D = Diaphragm: are the costophrenic and costocardiac margins sharp? is one hemidiaphragm enlarged over another? is free air present beneath the diaphragm? • E = Effusion/empty space: is either present? • F = Fields (lungs): are there infiltrates, increased interstitial markings, masses, air bronchograms, increased vascularity, or silhouette signs? • G = Gastric bubble: is it present and on the correct (left) side? • H = Hilar region: is there increased hilar lymphadenopathy?
Summarise as well! "The trachea is central, the mediastinum is not displaced. The mediastinal contours and hila seem normal. The lungs seem clear, with no pneumothorax. There is no free air under the diaphragm. The bones and soft tissues seem normal."
CASES Remember!: • Most disease states replace air with a pathological process • Each tissue reacts to injury in a predictable fashion • Lung injury or pathological states can be either a generalized or localized process
Evaluating an Abnormality 1. Identification of abnormal shadows 2. Localization of lesion 3. Identification of pathological process 4. Identification of etiology 5. Confirmation of clinical suspension • Complex problems • Introduction of contrast medium • CT chest • MRI scan
A single, 3cm relatively thin-walled cavity is noted in the left midlung. This finding is most typical of squamous cell carcinoma (SCC). One-third of SCC masses show cavitation
LUL Atelectasis: Loss of heart borders/silhouetting. Notice over inflation on unaffected lung
Atelectasis • Loss of air • Obstructive atelectasis: • No ventilation to the lobe beyond obstruction • Radiologically: • Density corresponding to a segment or lobe • Significant loss of volume • Compensatory hyperinflation of normal lungs
Consolidation • Lobar consolidation: • Alveolar space filled with inflammatory exudate • Interstitium and architecture remain intact • The airway is patent • Radiologically: • A density corresponding to a segment or lobe • Airbronchogram, and • No significant loss of lung volume
Cavitation:cystic changes in the area of consolidation due to the bacterial destruction of lung tissue. Notice air fluid level.
28 y/o female with sudden onset SOB while jogging this morning Well demarcated paucity of pulmonary vascular markings in right apex Left spontaneous pneumothorax