Download

1 / 22
220 likes | 492 Views
Neurologic and Musculoskeletal Imaging Studies. دکترامیر هوشنگ واحدی متخصص طب فیزیکی و توانبخشی قسمت 3. Sacroiliac joint imaging Anteroposterior angled and bilateral oblique views of the sacroiliac joints are the standard initial work-up. sacroiliac joint CT is higher sensitivity for

E N D
Neurologic and Musculoskeletal Imaging Studies دکترامیر هوشنگ واحدی متخصص طب فیزیکی و توانبخشی قسمت 3
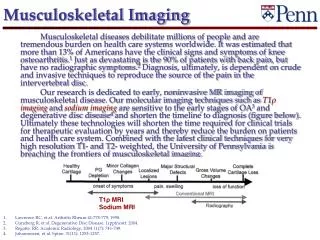
Sacroiliac joint imaging • Anteroposterior angled and bilateral oblique views of the sacroiliac joints are the standard initial work-up. • sacroiliac joint CT is higher sensitivity for • subtle erosive changes • detection of subtle sclerosis.
In the trauma setting, plain radiography is the initial imaging study. • CT can be considered in the setting of more complex acetabular and pelvic fractures to aid in surgical pIanning. CT is the preferred modality for assessment of osseous-based abnormalities of the hip • MRI is the preferred modality, following plain radiography, to image AVN, marrow replacement processes, musculoskeletal tumors, and osteomyelitis. • Magnetic resonance arthrography has a much higher accuracy than nonenhanced MRI in the detection and staging of acetabular labral lesions
The neck-shaft angle the collum-center-diaphysis or CCD angle is an important angle in the femoral neck.
Gage sign represents an area of lysis in the lateral epiphyseal margin and the adjoining metaphysis. this sign is indicative of a lateral deformation of the femoral head.
Knees • AP, lateral , both obliques • Patella • Lateral and tangential (sunrise) views • AP standing, AP standing with flexion, lateral, and patellar views • Additional techniques • Notch views • Stress views (varus, valgus, AP)
In the trauma setting, the minimum initial examination includes anteroposterior and lateral views. If there is a high clinical suspicion of fracture or lipohemarthrosis, then further views, such as bilateral oblique, sunrise, and/or tunnel notch, should be considered. Bone bruise or occult stress fracture are best shown with MRl.
The position of the patella is generally measured using the method described by Insall and Salvati , the ratio of the longest diagonal of the patella to the length of the patellar tendon should he between 0.8 and 1.2 .
The trochlear angle, the angle between the femoral condyles with its apex at the deepest point of the rochlear groove, is normally approximately 138°
Ankle &foot Ankle: anteroposterior (AP), lateral, mortise view Foot: standing AP, standing lateral, oblique AP, varus, valgus stress views Ligament injuries
A three-view plain radiography in patients with suspected ankle injury that includes • anteroposterior, • lateral, • and mortise views . • Fluoroscopy with stress views can be necessary to assess for Lisfranc fracture dislocations. • CT with reformations is often useful for preoperative planning in patients with complex comminuted fractures of the foot and ankle, and can alter clinical management. • chronic ankle pain, the ACR appropriateness criteria list plain radiographs as the initial imaging study, with magnetic resonance second for several.
Bones of the tarsals 7 tarsals 1- Talus 1- Calcaneus 1- Navicular 1- Cuboid 3- Cuneiforms
Interphalangeal angle This angle is used to evaluate interphalangeal hallux valgus.The longitudinal axes of the proximal and distal phalanx form an angle that should normally be less than 50.
Metatarsophalangeal angle Also referred to as the hallux valgus angle. The angle is formed by the longitudinal axes of the first metatarsal and the proximal phalanx of the first digit. Anangle of 150is regarded as normal; angles exceeding 150indicate a hallux valgus deformity.
The Philip-Fowler angle This angle is formed by the inferior calcaneus tangent and the tangent to the posterosuperior aspect of the tubercle of the calcaneus. Normal values for this angle range between 44° and 69°. An angle exceeding 75° is a sign of prominence of the tubercle of the calcaneus. Such a configuration is frequently associated with Achilles tendinitis or bursitis