Download
1 / 15
190 likes | 977 Views
Family Presence During Resuscitation. Shannon King, Leslee Johnson, Cydney Chomel, Amanda Lengerich, Kaitlyn Burke, Brooke Delay, Lindsey Gamrat, Nora Melvin, Hannah Crist, Kayelene Linkenheld. Background.

E N D
Family Presence During Resuscitation Shannon King, Leslee Johnson, Cydney Chomel, Amanda Lengerich, Kaitlyn Burke, Brooke Delay, Lindsey Gamrat, Nora Melvin, Hannah Crist, Kayelene Linkenheld
Background • In the past family members are taken to a waiting room during resuscitation (Boehm J., 2008) • If and when a nurse becomes available, the family may be updated on the patient’s status (Boehm J., 2008) • Recent debate has come up on inviting families in during resuscitation • Of families who have been apart of a code, 94% said they would do it again (Martin B., 2010)
Background • Nurses who invited families into the code were found to have increased self confidence (Twibell R., Siela D., Riwitis C., Wheatley J., Riegle T., Bousman D., & … Neal A., 2008) • In pediatric patients, families biggest stressor during a code was being separated from them (Maxton F. J. C., 2008) • Only 5% of Critical Care Units in the US have written policies about family presence during resuscitations (Martin B., 2010)
PICO Question • P- For families of Code Blue Patients • I- is being present during a resuscitation • C- compared to not being present • O- help the family cope with the event
Literature Review • “Family Presence During Resuscitation” • Level of evidence E: Evidence From Expert Opinions • Institutions need guidelines and should provide a support personal if family chooses to stay during resuscitation • Used several expert opinions and demonstrated the need for more research • Weaknesses of study: no actual experiment or study actually performed and there is limited knowledge regarding details of the practice (Engelhardt E., 2008)
Literature Review • “Should Families Be Present During Resuscitation?” • Level of evidence C: Systematic Review • Families should have the option to be present if appropriate • Looks at both the advantages and disadvantages • Looks at the family perspective and views, not just the patient • Weaknesses of the study: • No written policies • Hard to know if the patient wants family present (Fitzgerald K., 2008)
Literature Review • “Nurses' perceptions of their self-confidence and the benefits and risks of family presence during resuscitation” • Level of Evidence C: Qualitative • Majority agreed that family presence was a right of the family and the patient • Certified nurses and members of professional organizations perceived more benefits and fewer risks • Reluctance to family presence stems from • Unpleasantness of what the family sees • Fear that the team will not function as well • Anxiety that the family members will become disruptive • Family can see that everything was done to the patient to save the patient • Family can comfort the patient during resuscitation (Twibell et al, 2008)
Literature Review • 375 nurses participated in this qualitative study • 75% of the nurses had a least 6 yrs of experience • half of the study participants held a BSN degree • They used extensive statistical analysis on the survey responses • developed a tool that will allow the study to be repeated • Weaknesses of the study: • Single region (Ball Memorial Hospital Muncie, Indiana) • more than 95% were women • more than 90% were white • used convenience sampling (Twibell et al , 2008)
Literature Review • “Creating Advocates for Family Presence During Resuscitation” • Level of Evidence D: Peer Review • Uses different perspectives • Used national guidelines • Author has experience in codes • Medical Attitudes • Feel that family gets in the way, lack of knowledge, increased stress for both parties • Family Attitudes • Fear of the unknown, provide comfort, last chance to say goodbye • Weaknesses of the study: • Low level of evidence • Did not conduct own study (Agard, 2008)
Literature Review • “Parental Presence During Resuscitation in the PICU: The Parent’s Experience” • Level of evidence C: Qualitative Study • Being present lead to increased support from staff • Biggest stressor was being separated from their children • Parents felt “their role” was to be present • Purposive sampling was used • Worked with social workers to interview at appropriate times • Weaknesses of the study: • Small sample size • Study was voluntary (Maxton, 2008)
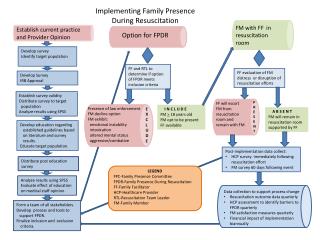
Implementations • Form a written policy • During admission, have a “Family Presence” form • Committee dedicated to family presence • Provide education (such as ELMS) to the staff • Assign role of facilitator for the family members • Evaluation post-implementation on all floors
AACN Audit of Family Presence During Resuscitation (Martin, 2010)
AACN Audit of Family Presence During Resuscitation (Martin, 2010)
References • Agard, M. (2008). Creating advocates for family presence during resuscitation.MEDSURG Nursing 17(3), 155-160. • Engelhardt, E. (2008). Family presence during resuscitation. The Journal of Continuing Education in Nursing, 39(12), 530. • Fitzgerald, K. (2008). Should families be present during resuscitation? MEDSURG Nursing, 7(16), 431-433. • Martin, B. (2010). Audit of family presence during resuscitation and invasive procedures, American Association of Critical Care Nurses. Retrieved from http://www.aacn.org/wd/practice/docs/practicealerts/family%20presence%20audit%20tool%204-2010%20final.pdf
References • Martin, B. (2010). Family presence during resuscitation and invasive procedures, American Association of Critical Care Nurses. Retrieved http://www.aacn.org/wd/practice/docs/practicealerts/family%20presence%2004-2010%20final.pdf • Maxton, F. J. C. (2008). Parental presence during resuscitation in the picu: the parents' experience. Journal of Clinical Nursing, 17, 3168-3176. doi: 10.1111/j.1365-2702.2008.02525.x • Twibell, R., Siela, D., Riwitis, C., Wheatley, J., Riegle, T., Bousman, D., & ... Neal, A. (2008). Nurses' perceptions of their self-confidence and the benefits and risks of family presence during resuscitation. American Journal Of Critical Care, 17(2), 101-112.