Download
1 / 39
390 likes | 517 Views
Valvular Heart Disease: No Longer the Realm of the Surgeon?. Christopher Young St Thomas’ Hospital, London. Outline. History, valve development and failure Surgical results and demographics Minimal Access (including robotic) Lessons to be learnt from surgery Summary and Conclusions.

E N D
Valvular Heart Disease:No Longer the Realm of the Surgeon? Christopher Young St Thomas’ Hospital, London
Outline • History, valve development and failure • Surgical results and demographics • Minimal Access (including robotic) • Lessons to be learnt from surgery • Summary and Conclusions
Bioprosthetic Problem Solving • Early • Calcification • Later valves • Tissue engineering (composite valves / muscle bar) • Zero pressure fixation • Anti-calcification remedies • Blue valves (toluidine blue) • Recent Valves • Sorin Valves (amino acids)
Significant Bioprosthetic Failures • Dura Mater – abandoned • Fascia Lata – abandoned • Ionescu-Shiley – abandoned • Autogenics - abandoned
Mechanism of Failure • Biological – gradual failure • Mechanical – catastrophic
Significant Failures • Mechanical • Bjork-Shiley • Duromedics • Abram’s Valve
Product Description Gore Thoracic Excluder Significant Failures – Endovascular Stents ePTFE Deployment Sleeve (attached to stent structure) • Gore Tag Self-expanding Nitinol Stent Structure Flares for wall apposition Radiopaque Band (both ends) ePTFE graft on blood-contact surface Sutureless Graft Attachment Spine Structure for Columnar Support Sealing Cuff (both ends)
Data from 5th National Adult Cardiac Surgical Database Report
Data from 5th National Adult Cardiac Surgical Database Report
Data from 5th National Adult Cardiac Surgical Database Report
Data from 5th National Adult Cardiac Surgical Database Report
Minimally Invasive Valve Replacement • Percutaneous peripheral cannulation • “Heartport” techniques • Mini-sternotomy • Mini anterior thoracotomy • Surgery under epidural anaesthesia
Robotic Aortic Surgery • 5 patients (3M/2F; 35 – 81 years) • 4 calcific AS / 1 AR • Transverse incision 4-5 cm R 3rd IC space • Standard interrupted suture technique • No mortality/complications • Mean hospital stay 8.6±3 days Folliguet et al. EJCTS 28 (2005): 172-173
Minimal Access Mitral Repair Port access CPB Endoclamp Multiple small incisions No rib spreading
Minimally Invasive vs Conventional Valve Replacement • Overall majority of reported results similar • Death • Length of stay • Complication rates • Minor negative aspects of: • Longer X clamp times • Longer bypass times • Increased early post-operative pain
Minimally Invasive vs Conventional Valve Replacement • Some reports of improved outcome with keyhole approach • Lower risk redo operations • Aortic vascular procedures • Lower transfusion requirements • Lower incidence post-operative AF • Lower post-operative pain after day 2
Off-Pump Valve Repair • Treatment of functional ischaemic MR • Coapsys device consists of 2 epicardial pads • Pads then connected with flexible chord • Placement TOE guided • MR reduced from grade 2.7±0.8 – 0.4±0.7 Grossi et al Ann Thorac Surg 2005; 80: 1706-11
The small annulus A tight squeeze
Small annulus • Good exposure from retraction sutures • Position light and table • Enthusiastic excision / decalcification • Do not oversize valve • Consider supra-annular placement • Do NOT use everting mattress sutures • (Root enlargement)
Summary 1 • Valve technology has evolved over 45 years with significant failures along the way (including recently) • Surgical results are excellent with increasing emphasis on minimal access
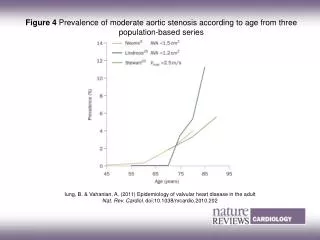
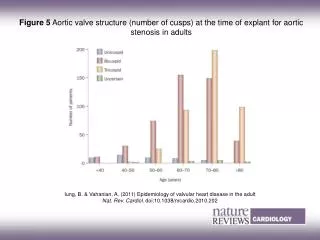
Summary 2 • Increasingly elderly population with more calcific disease • Surgical anatomy/pathology is varied; a “one size fits all” approach will not work • How long will the devices last and how will they fail?
Conclusions Proceed carefully! If things go pear-shaped Ring us – as usual, we will always be there to bail you out! This time, however, it may not be enough