Download
1 / 41
540 likes | 1.13k Views
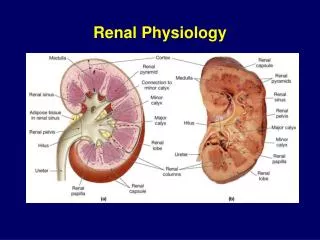
RENAL RADIONUCLIDE STUDIES Kateřina Michalová. Radionuclide diagnostics methods Noninvasive Are primarily physiologic Functional Does not provide the same anatomic details as morphologic method (X-ray,US,CT,MRI). Kupka K .a kol: Nukleární medicína, 2002. Nuclear renal imaging

E N D
RENAL RADIONUCLIDE STUDIES Kateřina Michalová
Radionuclide diagnostics methods Noninvasive Are primarily physiologic Functional Does not provide the same anatomic details as morphologic method (X-ray,US,CT,MRI) Kupka K .a kol: Nukleární medicína, 2002
Nuclear renal imaging • includes these methods • Renal dynamic scintigraphy • Renal cortical scintigraphy • Radionuclide Cystography
Dynamic renal scintigraphy Is a functional examination Providing information about intrarenal kinetics Of the i.v. applied radiopharmaceutical And of its transport via the efferent urinary tracts The specific information obtained depends of radiopharmaceutic injected.
Dynamic renal scintigraphy There are two kinds of Radiopharmaceticals: a) Tubular agents 99mTc-MAG3 Mercapto-acetyltriglycin 131I -,123I-Ortoiodhippurate b) Glomerular filtration rate agens 99mTc-DTPA Diethylentriamine pentaacetic acid
RadiopharmaceuticalsMechanisms of excretionyou can see in the picture Glomerular filtration • 99mTc DTPA Tubular secretion • 99mTc MAG3 • 131I, 123I – OIH Tubular fixation • 99mTc DMSA • 99mTc glucoheptonate
Radiopharmaceticals 99mTc-DTPA – Diethylentriamine pentaacetic acid belongs to the group of chelate compounds is excreted from kidneys through glomerular filtration with a half-life of 70 minutes it is the most suitable substance for measuring glomerular filtration (GFR) and good imaging of renal parenchyma Vižďa J. a kol : Atlas of Renal Scintigraphy, 2002.
Radiopharmaceticals • 99mTc-MAG3 - Mercapto-acetyltriglycine • is one of the newly developed radiopharmaceuticals • is rapidly excreted by the kidneys via active tubular secretion • and minor part via glomerular filtration • organic anions (which include MAG3) have a carboxyl group which specifically binds to the receptors of tubular cells mediating the active transport of MAG3 into the cells of the proximal tubulus • with normaI renal function 70% of the administered activity of the radiopharmaceutical (RP) is excreted within 30 minutes after the application
Dynamic renal study Radiopharmaceutical 99mTc - MAG3 Patient Preparation adequately hydration prior to the examination it is recommended to drink 100 ml of liquids per 10 kg of the body weight 30 min prior the examination empty bladder p.are requested to void completely prior to the study
Dynamic renal study Image Acquisition p.is usually examined in the supine position sometimes in sitting position detector of the gamma camera is in the posterior projection field of view includes the area of kidneys, ureters and the area of the bladder data recording startsimmediatelly before the intravenous injection as serial 15 sec images for 20 min radionuclide angiography 1 s frames are recorded for a period 1 minut after the administration of the RF can be used in examination of kidney grafts
Evaluation • visuel • parenchymal phase • position • size • shape • distribution RF • excretory phase • dilatation of the collecting system
Computer processing of the study Summed image of all frames during the clearance phase ROI (regions of interest) are drawn Renal ROI – arround the kidney Background ROI–below the kidney
Computer processing of the study Renogram curves Parameters of the curves Time activity curves derived from renal ROI Tmax = time of achieving the peak of the curve T1/2 = interval between the time of achieving the peak of the curve and the decrease to 50% of the peak level
Computer processing of the study quantitation of the individual renal function differential renal function DRF calculated within 1 to 3 minutes post injection of RP physiological range is 45%-55%
Normal renogram curve I. Vascular phase II. Secretory III. Excretory A II. III. I. čas
Patterns of renographic curves A obstructed pattern impaired renal function parenchymal lesion pattern renal failure patern normal renal failure pattern without measurable kidney uptake čas
Dynamic renal study Indications All uropaties, which require evaluation of individual renal function at diagnosis and during the different phases ofsurgical or conservative treatment and evaluation of the drainage function Examples include dilatation of the cause (e.g.Pelvi-Ureteric and Vesico-Ureteric dilatation), bladder dysfunction, complicated duplex kidney, post trauma, asymetrical renal function and reflux nefropathy.
Diuretic Renography The purpose of diuretic renography is to differentiate a true obstruction from a dilated non obstructed system (stasis) by serial imaging after intravenous administration of furosemide (Lasix)) 1) Standart renogram When dilatation of the collecting system exists, standart renogram should be complemented by a diuretic renogram 2) Diuretic renogram – additional 15-20 min acquisition, using the same technique as above Furosemid - 1mg/kg with a maximum dose 20mg(40 mg dle *SNM) *Society of Nuclear Medicine Procedure Guadeline for Diuretic Renography in Children
A obstruction no response to a diuretic no washout of RP from the collecting system non obstruction dilatation (hypotonie stasis) rapid washout from the collecting system Furosemid i.v. čas
Diuretic renography Indications differentiation obstructive from non obstructive causes of hydronephrosis and hydroureteronephrosis Ureteropelvic or ureterovesical obstruction Prenatal ultrasound diagnosis of hydronephrosis Post-surgical evaluation of the previously obstructed system Distension of pelvicalyceal system as an etiology of back pain
Left kidney -enlarged -dilated collecting system with pronounced retention of urine -response to the diuretic is rapid Right kidney normal shape collecting system with pronounced retentin of urine -response to the diuretic is rapid vertical position furosemid non obstruction dilatation (hypotonie stasis) rapid washout from the collecting system no obstruction
Left kidney -enlarged -dilated collecting system with pronounced retention of urine -poor response to the diuretic Right kidney washout of urine is free by nefrostomy vertical position furosemid obstruction poor response to a diuretic no washout of RP from the collecting system
Right kidney -enlarged hypofunctional impresion of dilatated collecting is seen, but no good fiiling no response to a diuretic Left kidney normal obstruction no response to a diuretic severe obstruction no response to a diuretic no washout of RP from the collecting system
Renal Cortical Scintigraphy Static imaging of the kidney Radiofarmaceutical : 99mTc-DMSA Dimercaptosuccinic acid Following iv injection is taken up into the renal cortex in the proximal convoluted tubule. The main site of accumulation are the microsomes of the cells of proximal tubules. It is cleared slowly , urine exrection is low.
Renal cortical scintigraphy Patient Preparation no Image Acquisition static high resolution images of kidneys (ANT, POST, RPO, LPO projection) SPECT in the supine position 2,5 h after injection DMSA cleared slowly (high radiation dose versus DRS !!!)
Renal cortical scintigraphy • Common Indications • Acute pyelonephritis • Renal scarring • Relativ functioning renal mass • Solitary or ectopic renal tissue (e.g.,pelvic kidney) • Horseshoe and pseudohorseshoe kidneys • Allergie to iodinated contrast agents • Society of Nuclear Medicine Procedure Guideline for Renal Cortical Scintigraphy in Children
Renal cortical scintigraphy - is used for detection of cortical defects of acute pyelonephritis (loss of function) and scarring related to chronic pyelonephritis. - is able to detect twice as many defects as ultrasound 4 times as many defects as intravenous urography - computed tomography has sensitivity and specificity similar but adds to the risk of contrast reaction and has a higher radiation exposure - magnetic resonance imaging is promising but expensive nonionizing method of vizualizing pyelonephritis Society of Nuclear Medicine Procedure Guideline for Renal Cortical Scintigraphy in Children
Normal renal scan ANT POST RPO LPO
Evaluation • number of kidneys • position • size • shape • the size, number and location of areas cortical loss • split renal function Note! Cortical „cold“ defect may be due to different etiology : tumor, abscess, cysts …. alrealdy is necesarry to compare with US
Evaluation of split renal function - for determination of percent differential function regions of interest of each kidney and background area are outlined on the computerized posterior and anterior images. • split renal function normally varies from 45%-55%
Acute pyelonephritis (multifocal) -more foci of reduced accumulation of the RP -diffuse damage to the parenchyma
Scarring characterized as : -wedshaped defects -with thinning or flattening of the cortex -irregular margins -loss of volume of the kidney ANT POST RPO LPO 2-years old girl after repeated infection of uropoetic system
Anomalies of position and number dystopia ANT POST
Direct Radionuclide Cystography Micturating cystography (MCG) -The examination is performed in the same way as X-ray MCG -Requires catheterization of the bladder and instilation of radionuclide and fluid for maximal physiological distension of the bladder, -Allowing imaging (dynamic scintigraphy) during filling, voiding, and after voiding. Radiopharmaceutical 99mTc- MAG3 Patient preparation no Time of examination 1 h
Direct Radionuclide Cystography • Common Indication • Screening and therapy monitoring vesicoureteral • reflux • Diagnostic offamiliar reflux • Evaluation of vesicoureteral reflux after medical management • Assesment of resuls of antireflux surgery • Comparing with conventional radiographic technique (X-ray MCG) • less gonadal radiation(100-200x lower than X-ray MCG) • higher sensitivityfor detectionof vesicoureteral reflux • does not provide the same anatomic details as X-ray MCG • Society of Nuclear Medicine Procedure Guideline for Radionuclide Cystography in Children
Direct Radionuclide Cystography Vezikoureteral reflux Interpretation criteria Grade I. with activity limited to the ureter II. with activity reaching the collecting system with none or minimal activity in ureter III. with a dilatation of the collecting system and dilated ureter Society of Nuclear Medicine Procedure Guideline for Radionuclide Cystography in Children
Visual evaluation Normal pattern no activity is recorded in the ureters
VUR grade III(into collecting system of the kidney with a dilatation)