Download
1 / 35
510 likes | 1.6k Views
Natural History of Achondroplasia. Autosomal Dominant Gene Mutation. Achondroplasia. The most common hereditary form of dwarfism. Incidence rate is between 1 in 15,000 and 1 in 40,000 live births.

E N D
Natural History of Achondroplasia Autosomal Dominant Gene Mutation
Achondroplasia • The most common hereditary form of dwarfism. • Incidence rate is between 1 in 15,000 and 1 in 40,000 live births. • It is a fully penetrant autosomal dominant disorder and the majority of cases (75-80%) are the result of a new (de novo) mutation.
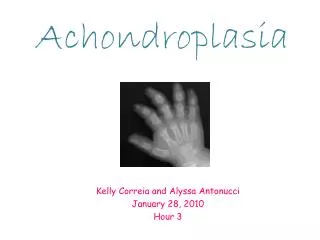
Achondroplasia • Affected individuals have short stature in arms and legs but not torso. • Other skeletal problems include trident hands, midfacial hypoplasia, prominent forehead (frontal bossing), thoracolumbar gibbus (hunched back), true megalencephaly, and narrowing of the spaces between the pedicles of the vertebra. • Overall survival and the average life expectancy for ACH population are decreased by 10 years. • ACH individuals are at greater risk for heart problems. • Bone abnormalities of the spine like narrow foramen magnum and spinal canal stenosis affect mortality at all ages but particularly in children. • Most individuals have normal intelligence.
Achondroplasia • Autosomal Dominant Point mutation in FGFR3 (Fibroblast growth factor receptor 3) • Gene located on Chromosome 4p16.3 • OMIM: #100800 • OMIM: *134934 • http://www.ncbi.nlm.nih.gov/entrez/dispomim.cgi?id=100800
Identifying Chromosomal Location of the ACH mutation • Velinov et al. (Nature Genetics 6, 314 - 317 (1994) ) mapped the achondroplasia gene near the telomere of the short arm of chromosome 4 (4p16.3), by family linkage studies using 14 pedigrees. • A positive lod score of z=3.35 with no recombinants was obtained with an intragenic marker for IDUA (Apha-L-Iduronidase) mapped earlier. • Shiang et al. and by Rousseau et al. used the “Candidate Gene Approach” to specifically identify the gene involved. • Look in the sequences in the region for a gene which could biologically make sense as the cause of Achondroplasia
Growth Factor • A naturally occurring protein capable of stimulating cellular proliferation and cellular differentiation. • Growth factors are important for regulating a variety of cellular processes by promoting cell differentiation and maturation. • Growth factors act as signaling molecules between cells by binding to specific receptors on the surface of their target cells.
Growth Factor Receptors • Receptors areprotein molecules embedded in either the plasma membrane or cytoplasm of a cell, to which a mobile signaling (or "signal") molecule may attach. • A molecule which binds to a receptor is called a "ligand," and may be a peptide (such as a neurotransmitter), a hormone, a pharmaceutical drug, or a toxin. • Growth Factor Receptors have Growth Factors as their ligands. • When the GF binds the receptor, a cellular response is initiated, resulting in cellular and developmental changes. Transmembrane Domain of a receptor usually has hydrophobic amino acid residues
What is a Fibroblast? • A type of cell that synthesizes and maintains the extracellular matrix of animal tissues. • Provides a structural framework for many tissues, and plays a critical role in wound healing. • The most common cells of connective tissue in animals. • Used in cell culture extensively.
There are Four Fibroblast Growth Factor Receptors • The FGF receptors bind to members of the fibroblast growth factor family of proteins. • Growth factors are proteins which attach to cell receptors, eliciting a response from the cell. This response varies depending upon the cell type, the receptor type, and the growth factor type. • FGF Receptors have an extracellular, binding domain with three immunoglobulin-like domains, a single helix domain that crosses the cell’s membrane, and an intracellular domain with tyrosine kinase activity.
Four different genes are currently known to encode distinct high-affinity FGF receptors.The 4.4-kb cDNA of the FGFR3 gene contains an open reading frame of 2520 nucleotides and consists of 19 exons and 18 introns.
There are at least 18 Fibroblast Growth Factors (FGF) • The FGFs regulate cell proliferation, differentiation, motility, and angiogenesis in embryonic development. • FGF growth factors bind to their FGF receptors in association with heparan sulphate proteoglycan (HSPG). When this happens, the receptors dimerize and phosphorylate themselves. • The dimers trigger phosphorylation (P) of downstream target proteins.
Phosphorylation • Protein kinases catalyze phosphorylation, and phosphatases reverse the process. • Adding a phosphoryl group can change a nonpolar hydrophobic protein into a polar, very hydrophilic molecule – in essence, changing its entire nature. • Each phosphorylation reaction and its reverse requires ATP to power it. • Tyrosine phosphorylation is not as common as other types of amino acid phosphorylation and can be studied with specific antibodies.
What is the Achondroplasia Mutation? • The mutation occurs in nucleotide position 1136 of the cDNA. The mutation is either a , a G-A transition or a G-C transversion on chromosome 4. • 150 of 154 unrelated achondroplasts had the G-A transition and only three had a G-C transversion at nucleotide 1138 of the FGFR3 gene. • Nucleotide 1138 of the FGFR3 gene is considered as the most sensitive point for germline mutation in the entire human genome. The mutation rate is estimated to be 0.000014 per gamete per generation.
Both mutations lead to the same Amino Acid substitution • Reverse Transcriptase PCR product was sequenced from heterozygous and homozygous ACH individuals revealed a point mutation within this region in the ACH individuals. • Both mutations result in the substitution of an arginine residue for a glycine at position 360 of the mature protein, which is in the transmembrane domain of FGFR-3. • A mother and daughter were reported with a new heterozygous double mutation at the same codon 380, which substituted a lysine instead of the usual arginine. These patients displayed a milder phenotype than the one encountered during achondroplasia
Increased Paternal Age is Associated with this Mutation • 80% of Achondroplasia occurs with no family history. The mutation is associated with an increased paternal age at the time of conception. It has been demonstrated that the mutated allele is always from a paternal origin. • Several diseases other than skeletal dysplasias are also associated with somatic mutations in FGFR3. • Seborrheic keratoses (skin growths) • Epidermal nevi (freckles) • Urothelial carcinomas (cancer of skin lining urethra)
RFLP Mapping can diagnose the two different mutations Fragment sizes: 57 bp 107 bp AGC TAC CGG GTG G to C transversion Msp I Fragment size 164 bp AGC TAC GGG GTG Normal Allele Fragment sizes 55 bp 109 bp AGC TAC AGG GTG G to A Transition Sfc I
RFLP of PCR Product • PCR products of 164 BP were amplified and electrophoresed on a 6% nondenaturing polyacrylamide gel. There are no Sfc l sites in the normal sequence in the FGF-DT PCR product. • However, the G+A transition mutation creates an Sfc l site that, if digested, results in fragments of 55 and 109 bp.
Role of FGFR3 in Development • Outside of the developing central nervous system, the highest level of FGFR3 mRNAs is in the prebone cartilage rudiments of all bones. • During endochondral ossification, FGFR3 is detected in resting but not growing (hypertrophic) cartilage.
Endochondrial Ossification: Conversion of Hyaline Cartilage to Bone Calcified cartilage forms Osteoblasts Chondroblasts http://en.wikipedia.org/wiki/Image:Bone_growth.png
Mutant Achondroplasia Mice have Skeletal Defects http://www.informatics.jax.org/greenbook/figures/figure8-1H.shtml
Homozygous Achondroplasia • The presence of two alleles for achondroplasia causes a serious skeletal disorder that leads to early death from breathing failure due to constriction by a tiny chest cage and neurological problems from hydrocephalus. • Homozygous achondroplasia, although fatal, has led to insights into other medical conditions. • Similarities were noticed between homozygous achondroplasia and a fatal condition of newborns called thanatophoric dwarfism. • Achondroplasia and thanatophoric dwarfism are due to different mutations in the FGFR 3 gene.
Other FGFR 3 Mutations Associated with Skeletal Defects TD = thanatophoric dysplasia, Craniosyn = craniosynostosis, Achon = achondroplasia, Hypochon = hypochondroplasia. Horton et al. 1998 Cells and Materials, 8: 83-87
Dwarf Horses and Dogs • Genetics of these animals is not due to the same mutation in FGFR 3 analagous gene.
http://www.cellmigration.org/resource/komouse/images/mousefig1.pnghttp://www.cellmigration.org/resource/komouse/images/mousefig1.png
Knockout Mice for Achondroplasia revealed New Insights • The knock-out mouse model is missing the FGFR 3 receptor. The negative regulation of bone formation is lost. The result is a mouse with excessively long bones and elongated vertebrae, resulting in a long tail. • Mutations of FGF3R confer a "gain of function". • It is proposed that the normal function of FGFR3 is to slow down the formation of bone by inhibiting the proliferation of chondrocytes, the cells that produce cartilage. • The mutation increases the activity of FGFR3, severely limiting bone growth.
Gain of Function Mutations • New or enhanced activity of a protein • Loss of function is more common mutation • Can you think of another Human mutation which could lead to a gain of new protein function?
Knockout Mice with excessively long bones, elongated vertebrae, long tails Deng et al. 1996 Cell, Vol. 84, 911–921
CATSHL Syndrome resembles Knockout Mice for FGFR 3 Toydemir, EM Am J Hum Genet. 2006 November; 79(5): 935–941.
Autosomal Dominant in CATSHL Pedigree Toydemir, EM Am J Hum Genet. 2006 November; 79(5): 935–941.
Current Medical Treatments for Achondroplasia • Surgical limb-lengthening procedures • Complications earlier, but more recently, more favorable and significant increases in height have been obtained over an 18-24-month period • Human growth hormone • Body disproportion reported, but more recently studies show improved height without adverse effect on trunk-leg disproportion Richette et al. Joint Bone Spine 75 (2008) 125-130
Future Therapies • Counteract the overactive FGFR3 effects on endochondral bone formation. • C-type natriuretic peptide (CNP) • Overexpression of CNP in mutant mice chondrocytes rescues achondroplasia through a MAPK-dependent pathway • Selective inhibition of the FGFR3 tyrosine kinase. • Drugs like imatinib used in cancer chemotherapy • blocking antibodies in order to interfere with binding of FGF ligands to FGFR3 Richette et al. Joint Bone Spine 75 (2008) 125-130
Prenatal Diagnosis and Genetic Counseling • Some obstetric risk for mother and child • Fetal diagnosis of achondroplasia is made with certainty when one or both parents have condition. • Diagnosis of achondroplasia is usually first suspected late in gestation on the basis of longbone foreshortening incidentally discovered by ultrasonography. • Disproportionately short limbs are seen in a heterogeneous group of conditions. Misdiagnosis can lead to inaccurate prenatal counseling. • Genetic confirmation can be performed with chorionic villi sampling or amniocentesis- with some risk to fetus. Recently a noninvasive maternal blood test has been developed. Richette et al. Joint Bone Spine 75 (2008) 125-130